Download
1 / 1
10 likes | 194 Views
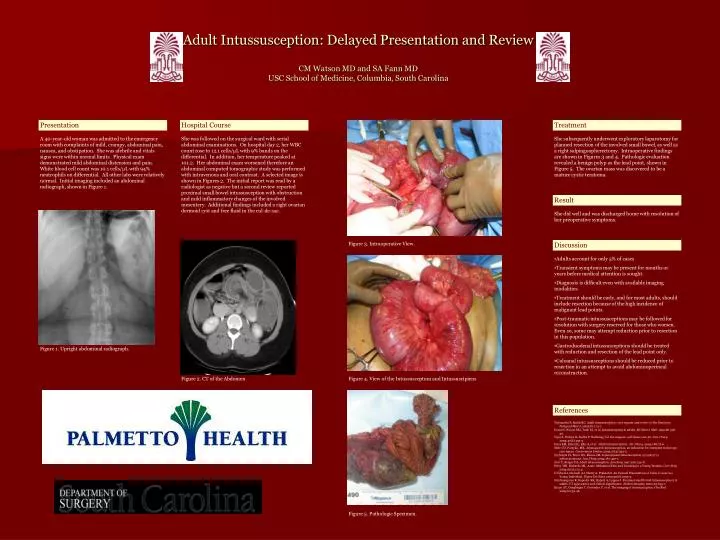
Adult Intussusception: Delayed Presentation and Review CM Watson MD and SA Fann MD USC School of Medicine, Columbia, South Carolina. Presentation. Hospital Course. Treatment.

E N D
Adult Intussusception: Delayed Presentation and ReviewCM Watson MD and SA Fann MDUSC School of Medicine, Columbia, South Carolina Presentation Hospital Course Treatment A 40-year-old woman was admitted to the emergency room with complaints of mild, crampy, abdominal pain, nausea, and obstipation. She was afebrile and vitals signs were within normal limits. Physical exam demonstrated mild abdominal distension and pain. White blood cell count was 10.1 cells/µL with 94% neutrophils on differential. All other labs were relatively normal. Initial imaging included an abdominal radiograph, shown in Figure 1. She was followed on the surgical ward with serial abdominal examinations. On hospital day 2, her WBC count rose to 12.1 cells/µL with 9% bands on the differential. In addition, her temperature peaked at 101.2. Her abdominal exam worsened therefore an abdominal computed tomographic study was performed with intravenous and oral contrast. A selected image is shown in Figures 2. The initial report was read by a radiologist as negative but a second review reported proximal small bowel intussusception with obstruction and mild inflammatory changes of the involved mesentery. Additional findings included a right ovarian dermoid cyst and free fluid in the cul-de-sac. She subsequently underwent exploratory laparotomy for planned resection of the involved small bowel, as well as a right salpingoopherectomy. Intraoperative findings are shown in Figures 3 and 4. Pathologic evaluation revealed a benign polyp as the lead point, shown in Figure 5. The ovarian mass was discovered to be a mature cystic teratoma. Result She did well and was discharged home with resolution of her preoperative symptoms. Figure 3. Intraoperative View. Discussion • Adults account for only 5% of cases • Transient symptoms may be present for months or years before medical attention is sought. • Diagnosis is difficult even with available imaging modalities. • Treatment should be early, and for most adults, should include resection because of the high incidence of malignant lead points. • Post-traumatic intussusceptions may be followed for resolution with surgery reserved for those who worsen. Even so, some may attempt reduction prior to resection in this population. • Gastroduodenal intussusceptions should be treated with reduction and resection of the lead point only. • Coloanal intussusceptions should be reduced prior to resection in an attempt to avoid abdominoperineal reconstruction. Figure 1. Upright abdominal radiograph. Figure 2. CT of the Abdomen Figure 4. View of the Intussusceptum and Intussuscipiens References Yalamarthi S, Smith RC. Adult intussusception: case reports and review of the literature. Postgrad Med J. 2005;81:174-7. Desai N, Wayne MG, Taub PJ, et al. Intussusception in adults. Mt Sinai J Med. 1999;66:336-40. Vijay S, Dahiya N, Sudha P. Radiology for the surgeon: soft tissue case 56. Can J Surg. 2004;47(6):453-5. Haas EM, Etter EL, Ellis S, et al. Adult intussusception. Am J Surg. 2003;186:75-6. Mele CD, Porayko, MK. Jejunogastric intussusception, an indication for emergent endoscopy: case report. Gastrointest Endosc 2003;57(4):593-5. Zeebregts CJ, Prevo RL, Klaase JM. Jejunojejunal intussusception secondary to adenocarcinoma. Am J Surg 2004;187:450-1. Azar T, Berger DL. Adult intussusception. Ann Surg 1997;226:134-8. Perry WB, Richards ML. Acute Abdominal Pain and Vomiting in a Young Woman. Curr Surg 2004;61(2);172-4. D’Silva KJ, Dwivedi AJ, Shetty A, Prakash S. An Unisual Presentation of Colon Cancer in a Young Individual. Digest Dis Scien 2005;50(6):1033-5. Sandrasegaren K, Kopecky KK, Rajesh A, Lappas J. Proximal small bowel intussusceptions in adults: CT appearance and clinical significance. Abdom Imaging 2004;29:653-7. Byrne AT, Goeghegan T, Govender P, et al. The imaging of intussusception. Clin Rad 2005;60:39-46. Figure 5. Pathologic Specimen.