Download
1 / 23
251 likes | 539 Views
Auer rods. Acute Leukemias Monday, October 13, 2003. Reading- Leukemia- AML and ALL (pp 40-43). Acute Leukemias. "AML" stands for Acute Myelogenous Leukemia Acute Myelocytic Leukemia Acute Myeloblastic Leukemia Acute Nonlymphocytic Leukemia (ANLL)

E N D
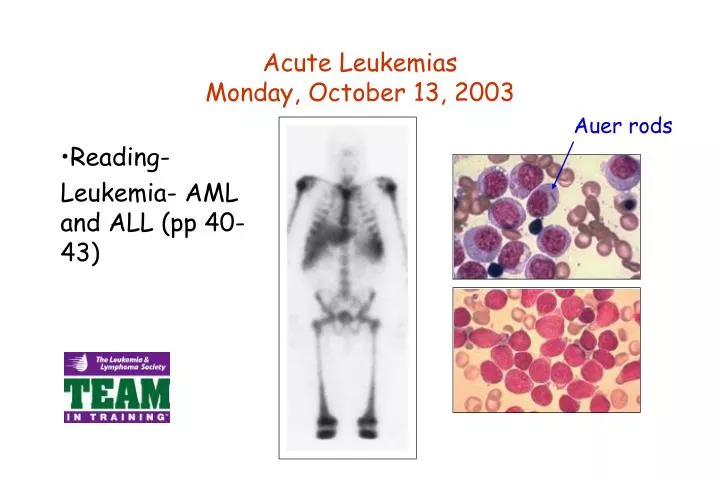
Auer rods Acute LeukemiasMonday, October 13, 2003 • Reading- Leukemia- AML and ALL (pp 40-43)
Acute Leukemias "AML" stands for Acute Myelogenous Leukemia Acute Myelocytic Leukemia Acute Myeloblastic Leukemia Acute Nonlymphocytic Leukemia (ANLL) •AML is a malignant clonal disorder originating from a deranged multipotent stem cell in some cases and from a unipotential progenitor cell in others. •AML is a continuous proliferation of abnormal blasts that fail to differentiate properly and they proliferate without maturing.
Cell of Origin •AML originates in many cases at a cell more mature than the pluripotent stem cell (PPSC), like committed progenitor cells. •Proliferation of defectivemyeloblasts, monoblasts, erythroblasts, or megakaryoblasts culminate in a pileup of incompetent blasts that dislodge normal marrow inhabitants.
Cell of Origin (cont’d) •The result is anemia, neutropenia, and thrombocytopenia; eventually the relentless overproduction of defective, immature cells may cause them to pour out into the bloodstream/lymph. •Although acute leukemia is traditionally associated with very high white cell counts, AML is first and foremost a marrow disease, with a lethal burden of >1012 tumor cells in 2-8 years. •Wide variability of the cell of origin of AML is likely to account for some of the striking morphological, molecular and clinical heterogeneity of AML.
Classification of AML •All cases of AML share many common biological features, but the morphology is strikingly heterogeneous. •FAB system (French-American-British) divides AML into seven (or eight) major groups and several subgroups. •The FAB system relies on: --identifying the lineage of the major population of blasts (myeloblast, monoblast, erthyroblast, or megakaryoblast), and --degree of differentiation.
Classification of AML (cont’d) •Other tests used to confirm or extend interpretation include: --cytochemical identification of myeloperoxidases; --staining with Sudan Black; and --periodic acid-Schiff (PAS)
FAB Classification for AML Class Alternative Bone Marrow Appearance M0/M1AML w/o most primitive, myeloblasts maturation predominate, little myeloperoxidase M2AML w/maturation >50% myeloblasts/promyelocytes Auer rods and myeloperoxidase activity. M3 Promyelocytic mainly promyelocytes, DIC from lysis of abnormal WBC's, Auer rods. M4 Myelomonocytic promonocytes and monocytes. M5Monocytic>80% monoblasts. M6Erthyroleukemia >50% bizarre nucleated RBC's M7Megakaryoblasticfibrosis in marrow, atypical megakaryocyte
Pathophysiology of AML •Most common complaints at presentation are fatigue, malaise, and a profound weakness worsening over 2-3 months. •Fever and night sweats, easy bruising (and petechiae) is sometimes present, but the traditional presenting complaints of cancer (weight loss and pain) are uncommon initially. •Acute leukemias cause morbidity/mortality 3 ways: --deficiency in normal blood cell or function; --invasion of vital organs with impairment of function; --systemic disturbances shown by metabolic imbalance.
Prognostic Indicators in AML Indicator Favorable Unfavorable Age <45 y.o. >60 y.o White cell count <25 x 109/L >100 x 109/L CNS disease absent present Auer rods present absent FAB type M3 or M4 M5, M6, M7 HLA DR negative positive TdT absent present Cytogenetics t(15;17) -7, del(7q)
Therapy of AML •2 basic types are used: cytotoxic chemotherapy; and post-ablation bone marrow transplantation. •Chemotherapy is the mainstay of management, but remissions are seldom permanent, side-effect are disheartening, and the 10 year "cure" rate is well under 20%. •Marrow transplantation can induce permanent remission in a substantial minority of patients, but is restricted in use by the need of compatible donor and prejudicial influence of age.
Definition of ALL ALL = Acute Lymphocytic Leukemia Acute Lymphoblastic Leukemia •Abnormalities of lymphoid cell differentiation/proliferation. ALL is a malignant disorder of lymphopoietic stem cells that originate in lymphoid precursors of marrow, thymus and lymph nodes. •ALL leukemic clones have heterogenous lineage and differentiation markers, and it has been difficult to classify. •The high frequency of ALL lymphoblasts that possess mixed phenotype markers indicate that the founding mutation may arise in the multipotent stem cell compartment.
A Curable Leukemia •Development of effective therapyfor patients with ALL is one of the undisputed successes of modern clinical hematology! •3 decades ago was uniformlyfatal, if left untreated the patient dies in ~6 months. •~70-80% of children and 20-30% of adults survive beyond 5 years; ~85% of the children who survive 10 years are considered "cured"; long-term "cure" in adults is unusual.
A Curable Leukemia (cont’d) •Pathophysiology was clarified and curative therapies found: --combinations of antileukemic drugs; --radiation; and supportive measures; --poor-prognosis ALL, goal is to intensify treatment to overcome drug resistance. Resulted in increasing the cure rate in children from 30% to 70%!; --patients withlesser risk, less intensive therapyhas resulted indecreased acute toxiceffects andimproved quality of life.
Cell Type •Transforming event in ALL can occur in any cell in the lymphoid pathway of hematopoietic stem cell differentiation: Children and Adults: >80% of pediatric cases involve B-cell progenitor cells; ~15% involve thymocytes; ~1% involve B-cells; <5% uncertain origin (have both T- and B-cell markers).
Cell Type (cont’d) Cell types: --progenitor B-cell ALL arises in the bone marrow; --B-cell ALL arises in lymphoid tissue; --T-cell ALL arises in the thymic or peripheral lymphoid tissue, often spreading to bone marrow.
FAB Classification for ALL •Leukemic lymphoblasts are morphologically indistinguishable from immature normal lymphoid cells. •Attempts to classify cells on size, nuclear/cytoplasmic ratio, presence of cytoplasmic granules, etc. have been unsuccessful! •FAB system has gained wide acceptance: --~90% of childhood ALL are FAB L1 subtype; small lymphoblasts with scanty cytoplasm and inconspicuous granules.
FAB Classification for ALL (cont’d) --L2 subtype, found in 5-15% of ALL cases; larger than the L1 cells, show marked variability in size, have prominent nucleoli and abundant cytoplasm --~1% of children have L3 lymphoblasts; appear identical to Burkitt's lymphoma cells •In adult ALL, distribution of FAB subtypes is different in that a much higher proportion of L2 subtypes is found.
Factors Predicting Event-Free Survival in Children with ALL Prognostic Factors Favorable Unfavorable Leukocyte Count <10 x 109/L >50 x 109/L Age 3 to 7 y.o. <1, >10 y.o. Sex Female Male Race Black White Immunologic markers early pre-B cell T cell, B cell FAB classification L1 L2, L3 Cytogenetic markers 6q- t(9;22)
Description of ALL •Clinical onset of ALL is usually acute and rapidly progressing. •Presenting symptoms are generally of short duration, and usually include fatigue, malaise, and a weary sense of health; ailing infants and children are irascible and touchy. •Fever and sweating are present in many patients, usually traceable to infection; skeletal pain is common but virtually any organ may become infiltrated by leukemic spread. •Following introduction of effective systemic chemotherapy, relapses were a problem-- the CNS and the testes are secure sanctuaries because of their protective blood barriers.
Therapy of ALL •In ALL, therapy is divided into 3 parts: --remission induction; --CNS prophylaxis; and --maintenance in remission. •Concept behind induction therapy is to destroy as many leukemic cells as possible as fast as possible by combination chemotherapy. •Although many of the agents used in managing ALL are identical to AML, several are selectively toxic to lymphoblasts; thus, long-term remission without severe marrow hypoplasia is achieved.