Download
1 / 82
820 likes | 968 Views
Central Nervous System Disorders. Rita Carey- N ita. Meningitis . Meningitis Inflammation of the brain & spinal cord due to viral or bacterial infection Bacterial is more serious & spread by direct contact with discharge from infected person

E N D
Central Nervous System Disorders Rita Carey-Nita
Meningitis • Meningitis • Inflammation of the brain & spinal cord due to viral or bacterial infection • Bacterial is more serious & spread by direct contact with discharge from infected person • Viral is more common & rarely serious AKA aseptic meningitis
Meningitis • Pathophysiology • Most common bacteria include: • Neisseria meningitis • Streptococcus pneumoniae • Haemophilus influenza type B • The infection generally begins in another area such as the respiratory tract then travels to the blood & invades the CNS • The meninges become inflamed & there is an increase in intracranial pressure • Vessel occlusion & necrosis of brain tissue may occur • Cranial nerve function may be impaired temporarily or permanently
Meningitis • Prevention • Vaccination is available to prevent Hib & S. pneumoniae • Early diagnosis & prompt treatment of individuals in contact with diagnosed patient is imperative
Meningitis Signs & Symptoms • Most common symptom: Headache • Caused by irritation of the dura mater & tension on blood vessels • High fever • Nuchal rigidity • Photophobia • Petechiae on skin & mucous membranes with meningococcal meningitis • Positive Kernig’s sign • Positive Brudzinski’s sign • Nausea & vomiting • Encephalopathy • Late signs: • Seizure • Lethargy
Meningitis • Complications • Need quick & effective treatment for positive resolution • Some patients have permanent neurological deficits while others recover completely • Some long term impairments include: • Blindness • Deafness • Seizures • Memory impairment • Learning disability
Meningitis • Diagnostic tests • Lumbar puncture • Viral: • clear CSF • normal glucose • normal to sl. protein • no bacteria • WBC count • Bacterial: • Turbid—cloudy • Massive WBC count • Identified by gram stain & culture • glucose • protein
Meningitis • Diagnostic Tests • Lumbar puncture with CSF analysis • CBC • C & S nose & throat • Done to determine complications • MRI • CT Scan
Meningitis • Therapeutic Interventions • Fatal if not treated promptly • Antibiotic therapy for bacterial meningitis • Symptoms management for both viral & bacterial • Decrease fever slowing to avoid shivering response • Antipyretics • Cooling blanket • Quiet dark environment to lessen stimulation • Analgesics for headache & neck pain • Corticosteroids & anti-inflammatory agents to decrease swelling • Anti-emetic to control nausea & vomiting • Safety in relation to seizures & agitation • Educate the family about symptoms & treatment • Isolation is required for patients with meningococcal meningitis to transmission to others
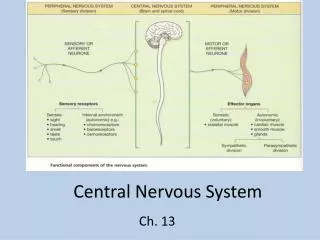
Encephalitis • Pathophysiology • Inflammation of the brain tissue • Neurological effect is dependent upon the area of nerve cell damage, necrosis or edema • Hemorrhage may occur with some types • Increased intracranial pressure with possible brain herniation may also occur
Encephalitis • Etiology • Viruses are the most common cause • West Nile—mononucleosis—mumps • Herpes Simplex Virus Type 1 is most common noninsectborne viral cause • unsure but virus may become active due to stress—fever—infectious disease • Parasites • Toxic substances • Bacteria • Vaccines • Fungi
Encephalitis • Signs & Symptoms • Headache & fever are the most common symptoms • Nausea • Vomiting • General malaise • Nuchal rigidity • Confusion • Decrease LOC • Seizure • Sensitivity to light • Ataxia • Abnormal sleep pattern • Tremors • Hemiparesis • Symptoms develop over several days
Encephalitis • Herpes encephalitis: • Edema & necrosis in the temporal lobe • at times associated with hemorrhage • Causes increase in intracranial pressure • Can lead to herniation of the brain • If patient is comatose before treatment the mortality rate is 70%-80% • Death occurs in first 72 hours when edema is worst
Encephalitis • Complications • Cognitive deficits • Personality changes • Seizures • Blindness • Diagnostic Testing • CT Scan • MRI • Lumbar Puncture with CSF analysis • CSF reveals WBC count & protein & normal glucose & yellow color due to breakdown of RBC’s • EEG
Encephalitis • Therapeutic Interventions • No treatment for insect borne encephalitis • Anticonvulsants • Antipyretics • Analgesics • Corticosteroids • Sedatives • Antiviral- acyclovior for herpes simplex
Increased Intracranial Pressure • Intracranial Pressure • The pressure exerted within the cranial cavity by the brain, blood & CSF • Any increase in one of the components without decrease in another results in increase ICP • Normal intracranial pressure is 0-15 mmHg • Fluctuates normally with changes in position—arterial pulsations—increases in intrathoracic pressure • Causes of increased intracranial pressure: • Brain injury—intracranial hemorrhage—brain tumor • Outcome & deficit is dependent on the degree of elevation & speed of increase in ICP • Early detection & intervention is imperative
Increased Intracranial Pressure • The body will compensate: • CSF will be shunted to the subarachnoid space in the spinal column • The cerebral vessels will constrict decreasing the amount of blood in the brain • Only temporary & not effective for sudden & severe increases in ICP
Increased Intracranial Pressure • Signs & Symptoms • Initial symptoms are • Restlessness—irritability—decreased level of consciousness • Hyperventilation causing vasoconstriction • Increasing temperature • Vomiting • Headache • Dilated pupil on affected side with progression of bilateral fixed & dilated pupils • Hemiparesis or hemiplegia • Decorticate then decerebrate posturing • Late signs include Cushing Triad: • Bradypnea—bradycardia—arterial hypertension creating widened pulse pressure • Interventions may not be successful at this point
Increased Intracranial Pressure • Nursing interventions: • HOB 30 degrees • Avoid flexion of neck & hip • Administer antiemetics • Administer antitussives • Administer stool softeners • Minimal suctioning • Decrease noise & unnecessary stimuli • Provide rest periods
ICP Monitoring • ICP Monitoring: • Detects early changes before symptomatic • Placement of catheter into ventricles of brain, parenchyma or subdural or subarachnoid space • Done at bedside or surgically • Scalp anesthetized & burr hole drilled into skull • External ventricle drainage • Catheter placed in the lateral ventricles • Allows for pressure monitoring • Drains CSF to reduce increase in ICP • Disadvantages: • Difficult insertion of catheter • Clotting of catheter by blood in CSF
ICP Monitoring • Subarachnoid Bolt • Tightly screwed bolt into burr hole after the dura has been punctured • Ease in placement • Disadvantages • Occlusion of sensor portion of bolt by brain tissue • Inability to drain CSF • Intraparenchymal monitor • Monitor is placed directly into brain tissue • Most accurate reflection of ICP • Disadvantages • Does not drain CSF • May become occluded by brain tissue
ICP Monitoring • Patients are generally in ICU • They are mechanically ventilated, pharmacologically paralyzed & sedated • Provided family with support & education
Nursing Implications for patients with infectious & inflammatory neurological disorders • Obtain history from patient or significant other • Ascertain any risk or events that could contribute • Thorough physical assessment with extensive neurological focus • LOC—pupillary reaction—orientation—muscle strength • Assess for signs & symptoms of ICP • Monitor vitals • Assess pain level on scale 0-10 & provide analgesic as necessary • Keep HOB 30 degrees • Provide quiet dim environment • Decrease exposure to stimuli • Position for comfort, prevention of pressure ulcer & contractures • Monitor for safety • Seizure precaution • Decreased level of consciousness • Alteration in mental status • Educate & involve family in care
Headaches • Headaches are a common symptom of neurological disorders • Most are transient • Recurrent, persistent & increasing severity warrant further neurological evaluation • Types • Tension or Muscle Contraction • Migranes • Cluster
Tension or Muscle Contraction Headache • Tension or Muscle Contraction Headache • Persistent contraction of scalp, facial, cervical & upper thoracic muscles are cause • Cycle of muscle tension & muscle tenderness occurs • May or may not be accompanied by vasodilation of cerebral arteries • Associated with • PMS—anxiety—stress—depression • Symptoms develop gradually with radiation of pain from crown of head to base of skull • Variation of location & intensity • Pressure—aching—tight are words often used to describe headache • Treatment includes • Relaxation techniques—massage—nonnarcotic analgesics—counseling
Migraine Headaches • Migraine Headaches • Caused by the cerebral vasoconstriction followed by cerebral vasodilation • May be triggered by • Trigeminal nerve stimulating release of substance P, a pain transmitter, into the vessels • Release of serotonin—norepinephrine—epinephrine • Aura may or may not occur • Hereditary tendency • Throbbing—viselike—pounding are terms used to describe • Noise & light tend to exacerbate • Triggers include • Noise—alcohol—bright light—specific food
Migraine Headaches • Two types: • Classic & common • Classic Migraine • Has prodromal phase • Visual disturbance—difficulty speaking—numbness & tingling • Headache follows accompanied by nausea & sometimes vomiting • Last hours to days • Common Headache • Does not have prodromal phase • Immediate onset of throbbing headache
Migraine Headaches • Treatment • Prophylactic or Acute • Prophylactic • Dietary restriction of precipitating food & beverages • Nifedipine (calcium channel blocker) & propranolol (beta-andrenergic) to control blood pressure & prevent vascular changes • Amitriptyline (tricyclic antidepressant) • Acute • Ergot (Cafergot) a vasoconstrictor is effective if taken within 30-60 minutes of onset • Imitrex & Zomig work at serotonin receptor sites & have vasoconstricting effect
Cluster Headaches • Cluster headaches causes • Vascular disturbances—stress—anxiety—emotional distress • Occur in clusters that span from several days to weeks • Episodes may not occur for months to years • Alcohol worsens episodes • Throbbing—excruciating are terms used to describe • Unilateral affecting the nose—eye—forehead • Affected eye is bloodshot & teary
Cluster Headaches • Treatment is difficult & includes • Quiet dark environment • Cold compress • NSAIDS • Tricyclic antidepressant • Diagnosis • Based on patient’s history & symptoms • MRI—CT scan—EEG—arteriogram—cranial nerve testing—lumbar puncture to test CSF • may be done to rule out other causes
Assessment of Headache • Assessment should include: • Rate pain on scale of 0-10 • Describe the quality of pain? • Where is pain? • Does pain start in one place? Does it radiate? • What aggravate & alleviates pain? • When is it experienced? • PMS—emotional stress—tension • Any associated symptoms • Nausea—vomiting—bloodshot eyes
Nursing Interventions • Quiet dark environment • Relaxation techniques & stress reduction • Identify precipitating factors through recording • Time of onset • Aggravating factors • Food eaten • Associated symptoms • Reduce or eliminate • Provide patient education about medication
Seizure Disorder • Seizure • Sudden, abnormal & excessive electrical discharges from brain that can change motor or autonomic function, consciousness or sensation • Can occur at any time in life • Can occur at any time • May be a symptom of epilepsy or some other neurological disorder such as brain tumor or meningitis • Epilepsy • Chronic neurological disorder characterized by recurrent seizure activity
Seizure Disorder • Pathophysiology • Neuron membrane is instable • Instability allows for abnormal electrical discharge • Classified as: • Partial • Generalized • Partial • Begin on one side of cerebral cortex & sometimes spreads to the other hemisphere becoming generalized • Generalized involves both cerebral hemispheres
Seizures • Etiology • May be acquired or idiopathic • Causes include: • Brain injury—anoxia • Onset before 20 is idiopathic • New onset after 20 is usually caused by underlying neurological disorder • Signs & Symptoms • Depends on area of brain where seizure begins • Some people experience aura prior • If aura experienced it serves as warning of onset
Partial Seizure • Classic symptoms: • Repetitive—purposeful behaviors • Called automatisms • Dreamlike state while automatisms occurring • Lip smacking—picking at clothes—chewing—spitting—fondling self • Pt unaware of behaviors • Simple partial seizure if no lose of consciousness & less than 1 minute long • Complex seizure or psychomotor seizure if consciousness lost & lasts 2-15 minutes
Partial Seizure • Origin • Parietal lobe—paresthesias on opposite side of body from seizure focus • Occipital lobe—visual disturbances • Motor cortex—involuntary movement in arm or hand to leg & face on opposite side of seizure focus
Generalized Seizure • Generalized • Affects entire brain • Two types • Absence seizures • Tonic-clonic seizures • Absence seizures • AKA petit mal seizure • Occur primarily in children • Period of staring that last several seconds
Tonic-clonic seizure • Tonic-clonic • AKA grand mal seizures or convulsions • Aura & loss of consciousness may occur • Tonic phase: • 30-60 seconds • Rigidity—pupils fixed & dilated—hands & jaw clenched—period of apnea • Clonic phase: • Contraction & relaxation of all muscles in jerky rhythmic pattern • Extremities move forcefully causing possible injury if environment not clear • Incontinence • Biting of lip or tongue can occur
Postictal Period • Postictal period: • Recovery period after seizure • Partial seizure: • postictal period last only few minutes • Disorientation noted • General seizure: • Postictal period may last 30 minutes to several hours • Deep sleep • Followed by headache—confusion—fatigue • Patient may realize they had seizure but not remember event
Diagnostic Tests • EEG • Most useful diagnostic test • Determines: • where in brain seizure start • Frequency & duration of seizure • Presence of asymptomatic seizures • Sleep deprivation & light stimulation may be used to evaluate seizure threshold
Therapeutic Interventions • If there is a cause for the seizure then the focus is on treating cause • If there is no apparent cause the focus is on controlling the seizure activity • Anticonvulsant medications utilized • Start pt on one with dose increased until therapeutic with minimal side effects • If not controlled another medication is added • Renal & hepatic function are monitored • Drowsiness is common side effect so educated pt to avoid driving until effect of drug is known • Driving is contraindicated until seizures are controlled • Must wean off any seizure medication to avoid status epilepticus
Surgical Management • Surgery may be required if medication is not effective • May have area of seizure resected if within nonvital brain tissue • May reduce seizure activity or cure • If unable to identify focus area or if the focus is in vital area such as motor cortex or speech center surgery is not an option
Emergency Seizure Care • Main goal is to prevent injury • Seizure precautions: • Padded side rails • Call bell in reach • Assist with ambulation • Keep suction & airway at bedside
Emergency Seizure Care • Nursing Care During Seizure: • Clear environment if seizure occurs & patient on floor • Loosen restrictive clothing • Turn patient on side to maintain airway & prevent aspiration • Do not force anything into airway once the seizure has started • Do not restraint patient • Monitor vitals if possible • Observe & document: • Behavior during • Which part of body involved • Progression of seizure • Length of seizure
Emergency Seizure Care • After the seizure • Monitor vitals • Assess breathing • Suction if necessary • Rescue breathing or CPR if necessary
Status Epilepticus • Status epilepticus • Seizure activity lasting at least 30 minutes without return to consciousness • Medical emergency requiring prompt intervention to prevent irreversible neurological damage • Main cause is abrupt cessation of anticonvulsant medication
Emergent Medical Intervention • Need adequate oxygen so may be intubated & mechanically ventilated • Intravenous diazepam or lorazepam to stop seizure • Need to monitor resp depressive affects of these medications • Serum drug levels of anticonvulsants are reviewed & medication is adjusted to therapeutic level • If seizures continue: • Barbiturate coma induced with intravenous penobarbital • Last resort • Anesthesia or pharmacological paralysis requiring intubation, mechanical ventilation & management in ICU
Emergent Medical Intervention • Continuous EEG monitoring is done to determine seizure activity has stopped • A neuromuscular blockade will have to visible signs of seizure but continue to seize
Psychosocial Effects • Most patient’s with seizure control live normal productive lives • Patient may be embarrassed by seizure activity • Incontinence—involuntary movement—sounds made • Affects financial aspects • Denied insurance so need to pay out of pocket • Job opportunities may be limited due to job safety or transportation issue • Interpersonal relationships may suffer • Fear of possible seizure activity in front of friend or partner • Lower self esteem