Download
1 / 1
70 likes | 373 Views
Vanderbilt Pediatric Hematology Thrombosis Protocol . 4 / 11 / 12. Robert F. Sidonio, Jr. MD, MSc . . Yes. Candidates for anticoagulation thromboprophylaxis Elevated lipoprotein (a) Protein S/C deficiency Antithrombin deficiency Antiphospholipid antibody syndrome

E N D
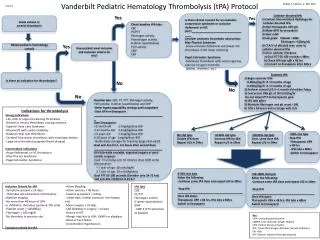
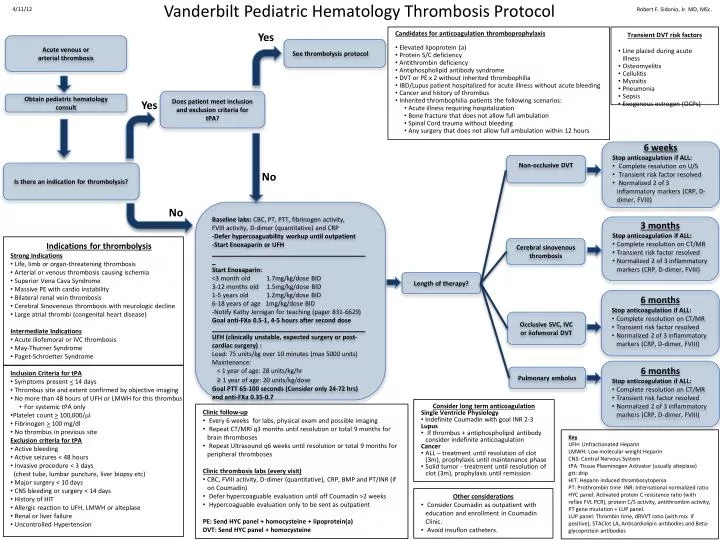
Vanderbilt Pediatric Hematology Thrombosis Protocol 4/11/12 Robert F. Sidonio, Jr. MD, MSc. Yes • Candidates for anticoagulation thromboprophylaxis • Elevated lipoprotein (a) • Protein S/C deficiency • Antithrombin deficiency • Antiphospholipid antibody syndrome • DVT or PE x 2 without inherited thrombophilia • IBD/Lupus patient hospitalized for acute illness without acute bleeding • Cancer and history of thrombus • Inherited thrombophilia patients the following scenarios: • Acute illness requiring hospitalization • Bone fracture that does not allow full ambulation • Spinal Cord trauma without bleeding • Any surgery that does not allow full ambulation within 12 hours • Transient DVT risk factors • Line placed during acute illness • Osteomyelitis • Cellulitis • Myositis • Pneumonia • Sepsis • Exogenous estrogen (OCPs) Acute venous or arterial thrombosis See thrombolysis protocol Does patient meet inclusion and exclusion criteria for tPA? Obtain pediatric hematology consult Yes • 6 weeks • Stop anticoagulation if ALL: • Complete resolution on U/S • Transient risk factor resolved • Normalized 2 of 3 inflammatory markers (CRP, D-dimer, FVIII) Non-occlusive DVT Is there an indication for thrombolysis? No No Baseline labs: CBC, PT, PTT, fibrinogen activity, FVIII activity, D-dimer (quantitative) and CRP -Defer hypercoaguability workup until outpatient -Start Enoxaparin or UFH _____________________________________________ Start Enoxaparin: <3 month old 1.7mg/kg/dose BID 3-12 months old 1.5mg/kg/dose BID 1-5 years old 1.2mg/kg/dose BID 6-18 years of age 1mg/kg/dose BID -Notify Kathy Jernigan for teaching (pager 831-6629) Goal anti-FXa 0.5-1, 4-5 hours after second dose ____________________________________________ UFH (clinically unstable, expected surgery or post-cardiac surgery) : Load: 75 units/kg over 10 minutes (max 5000 units) Maintenance: < 1 year of age: 28 units/kg/hr ≥ 1 year of age: 20 units/kg/dose Goal PTT 65-100 seconds (Consider only 24-72 hrs) and anti-FXa 0.35-0.7 • 3 months • Stop anticoagulation if ALL: • Complete resolution on CT/MR • Transient risk factor resolved • Normalized 2 of 3 inflammatory markers (CRP, D-dimer, FVIII) • Indications for thrombolysis • Strong Indications • Life, limb or organ-threatening thrombosis • Arterial or venous thrombosis causing ischemia • Superior Vena Cava Syndrome • Massive PE with cardio instability • Bilateral renal vein thrombosis • Cerebral Sinovenous thrombosis with neurologic decline • Large atrial thrombi (congenital heart disease) • Intermediate Indications • Acute iliofemoral or IVC thrombosis • May-Thurner Syndrome • Paget-Schroetter Syndrome Cerebral sinovenous thrombosis Length of therapy? • 6 months • Stop anticoagulation if ALL: • Complete resolution on CT/MR • Transient risk factor resolved • Normalized 2 of 3 inflammatory markers (CRP, D-dimer, FVIII) Occlusive SVC, IVC or iiofemoral DVT • 6 months • Stop anticoagulation if ALL: • Complete resolution on CT/MR • Transient risk factor resolved • Normalized 2 of 3 inflammatory markers (CRP, D-dimer, FVIII) • Inclusion Criteria for tPA • Symptoms present <14 days • Thrombus site and extent confirmed by objective imaging • No more than 48 hours of UFH or LMWH for this thrombus • For systemic tPA only • Platelet count > 100,000/l • Fibrinogen > 100 mg/dl • No thrombus in previous site • Exclusion criteria for tPA • Active bleeding • Active seizures < 48 hours • Invasive procedure < 3 days • (chest tube, lumbar puncture, liver biopsy etc) • Major surgery < 10 days • CNS bleeding or surgery < 14 days • History of HIT • Allergic reaction to UFH, LMWH or alteplase • Renal or liver failure • Uncontrolled Hypertension Pulmonary embolus • Consider long term anticoagulation • Single Ventricle Physiology • Indefinite Coumadin with goal INR 2-3 • Lupus • If thrombus + antiphospholipid antibody consider indefinite anticoagulation • Cancer • ALL – treatment until resolution of clot (3m), prophylaxis until maintenance phase • Solid tumor - treatment until resolution of clot (3m), prophylaxis until remission • Clinic follow-up • Every 6 weeks for labs, physical exam and possible imaging • Repeat CT/MRI q3 months until resolution or total 9 months for brain thromboses • Repeat Ultrasound q6 weeks until resolution or total 9 months for peripheral thromboses • Clinic thrombosis labs (every visit) • CBC, FVIII activity, D-dimer (quantitative), CRP, BMP and PT/INR (if on Coumadin) • Defer hypercoaguable evaluation until off Coumadin >2 weeks • Hypercoaguable evaluation only to be sent as outpatient • PE: Send HYC panel + homocysteine + lipoprotein(a) • DVT: Send HYC panel + homocysteine Key UFH: Unfractionated Heparin LMWH: Low molecular weight Heparin CNS: Central Nervous System tPA: Tissue Plasminogen Activator (usually alteplase) gtt: drip HIT: Heparin induced thrombocytopenia PT: Prothrombin time INR: International normalized ratio HYC panel: Activated protein C resistance ratio (with reflex FVL PCR), protein C/S activity, antithrombinactivity, PT gene miutation+ LUP panel. LUP panel: Thrombin time, dRVVT ratio (with mix if positive), STAClot LA, Anticardiolipin antibodies and Beta-glycoprotein antibodies • Other considerations • Consider Coumadin as outpatient with education and enrollment in Coumadin Clinic. • Avoid insufloncatheters.