Download

1 / 42
420 likes | 633 Views
Burn –4 th lecture. WOUND HEALING AND THE BIOLOGY OF SCAR (SCAR FORMATION). Types of the body tissues: There are four types of tissues in the body: Epithelial tissue as the stratified squamous epithelium of the epidermis of the skin. Connective tissues which are 3 types:

E N D
Burn –4thlecture WOUND HEALING AND THE BIOLOGY OF SCAR (SCAR FORMATION)
Types of the body tissues: There are four types of tissues in the body: • Epithelial tissue as the stratified squamous epithelium of the epidermis of the skin. • Connective tissues which are 3 types: a. Connective tissue proper with soft matrix b. Cartilage with rubbery matrix. c. Bone with solid matrix. 3. Muscular tissues. 4. Nervous tissues. Connective tissue proper: Proper C.T. are the supportive tissues, any C.T. is formed of 3 parts: a.Cells which are called the C.T. cells. b. Fibers which are called the C.T. fibers. c. Matrix: soft ground substance.
Proper connective tissue cells as fibrocyteand mast cell: Fibroblast or fibrocyte: is the most important and commonest C.T. cell which is responsible for the formation of the C.T. fibers and repair of injuries. Mast cell:oval or rounded in shape, its cytoplasm is rich in granules, its nucleus is small, central and rounded. Mast cells secrete heparin, which is anticoagulant as well as the chemotactic factor as histamine to stimulate the chemosensitive pain receptors. Mast cells usually present around blood vessels. Connective tissue fibers are: • Collagenous fibers. • Elastic fibers. • Reticular fibers.
White collagenous fibers: are formed of protein called collagen, which is glue-like substance arranged in bundles. Yellow elastic fibers: are elastic in nature (stretchable), and formed of protein called elastin. Reticular fibers: are formed of protein called reticulin, reticular fibers are arranged in the from of fine network. Matrix: ground interstitial substance: the C.T. cells and the C.T. fibers are embedded in a soft gelly-like substance called the matrix.
Functions of the proper C.T • It support and connect the different organs & Tissues together. • The matrix acts as medium for transport of nutrition. • Specific function for each fiber & cell. As Fibroblast cell are responsible for C.T fiber formation & injuries repair, mast cells release heparin & chemotactic factors, Elastic fiber gives Elasticity, collagen fibers gives strength, while pigment cells are responsible for melanin production. Repair of wounds The healing of skin wound requires 2 processes: • Regeneration of the epidermis • Fibrosis in the dermis
There are 2 types of wound healing: 1. Primary union of wound = healing by first intention: As the surgical incision healing where no epithelial loss. This Occurs in clean surgical wounds with closely approximated in edges, incision and sutures induce inflammation in both edges. Within 24 hours the basal cell layer of the epidermis regenerate and cover (bridge) the wound surface, subsequently other epidermal layers (superficial ones) regenerate with more covering of the wound surface.
Fibroblasts on both sides of the wound proliferate(they received blood & nutrients from the endothelial capillaries = Neovascularization = capillary sprouting) Fibroblasts proliferate & from granulation tissues, which close the wound within 4-5 days, but union, still weak. Fibroblasts lay down collagen (glue), CAPILLARIES BECOME obliterated and the granulation tissue (weak) changed into solid fibrous Tissue (Scar=cicatrix). The wound edges are now firmly united, the covering epidermis is pale and dose not have hair follicles, sweat or sebaceous glands.
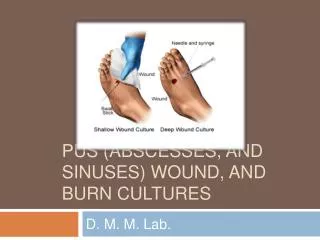
2-Secondary union of wounds = healing by 2nd intention: Where there is epithelial loss. This Occurs in septic or open wounds with separated edges. Formation of new capillaries (Neovascularization) proliferation of Fibroblasts -> granulation weak tissue takes place all around the cavity of the wound. Infection of wound causes emigration of a large number of neutrophils to the wound area leading to exudation of fluid from the septic granulation tissue (pyogenic membrane = pus), once the infection is overcomed, the granulation tissue becomes healthy and resist further infection.
Then capillary loops will be formed at the bottom of the wound cavity —> granulation tissue which is red, moist, insensitive to touch and bleeds easily, and gradually these granulation tissues will fills up the cavity. When the cavity is completely filled up with granulation Tissue -> the epidermis will grows from the edges. Finally granulation weak tissue will be changed into solid fibrous tissue (big scar devoid of hair & glands).
Complications of 2ndry union: • Chronic ulcer: in a wide wound, cicatrization occurs at the bottom before the cavity is filled up with granulation tissue -and this will hinder the healing process -> ulcer. • Sinus or Fistula. • Massive outward growth of granulation tissue -> hinder epithelization. • Keloid formation: Keliod = Excessive formation of solid fibrous Tissue in the dermis leading to projecting swelling covered by thin epidermis, recurrence of keliod after surgical removal is common. Keloid develops during the healing of burn or smallpox vaccination vesicles.
Biology of the scar formation Scar, which is the glue of our body, is formed through a highly organized sequence of physiological events. A knowledge of wound healing enables the physiotherapist to design and implement treatment strategies based on scar biology. The basic definition of wound is the disruption of unity. Primitive animals respond to injury by mitosis of their cells (they are capable of regenerating or duplicating their missing parts). Selected organs in our body still retain this biological gift of regeneration's in cases of scratches and mild burns of the skin where healing occurs by epidermal regeneration. Also Hepatocytes of the liver are capable of regrowth following mild toxic conditions, as well as peripheral nerves heal by axonal regeneration dusty to restore nerve tracts.
Ability of these tissues to regenerate or reduplicate is limited only to minor injuries, and not to more devastating injuries as full - thickness burns, liver cirrhosis and large nerve gaps, where another mean of repair will take place in all vertebrates, in which special cells will respond to injury by forming the collagenous (glue), this body glue is called the granulation scar tissue. Our body has at least "14" different types of collagen, the most important one of them is (type I collagen) which is responsible for the formation of the mature scar. Type I collagen is called the chameleon collagen due to its ability to imitate the structure of the other collagen types.
Phases of wound healing There are 3 phases of wound healing: • Inflammatory phase: which prepares the area for healing. • Fibroblastic phase: which rebuilds the structure. • Remodeling phase: which is the final from.
1-Inflammatory phase: Inflammatory is normal and necessary for the healing process, any blood vessels that traversed the wound will be cut at the time of injury. These cut vessels will pour blood in to the wound, then blood will be coagulated with sealing off the injured vessels and lymphatic channels leading to temporary closing of the wound injured vessels as well as mast cells in the injured tissue will release histamine, which will lead to vasodilatation of the neighboring non-injured vessels also there is a release bradykinins,prostaglandins and other proteglycans with more vasodilatation & edema creating a red, hot swollen and painful condition.
This inflammation (V.D & swelling) is inevitable and needed for healing but balance of this inflammation is also needed because: • If there is no inflammation —> there is no healing, • Too little inflammation -» slow healing, • Balanced inflammation -> proper & good healing, • Too much inflammation -> excessive scar formation,So excessive swelling & inflammation must be prevented Via: Medically: by repairing & cauterization of all blood vessels Therapeutically: by the classic (RICE) regime of rest, Ice, compression and elevation. Pharmacologically: by using steroids & Aspirin which inhibits the prostaglandin release.
Under the umbrella of the inflammatory phase, there are 2 processes: a. Phagocytosis b. Neorvascularzation.
A) Phagocytosis = wound decontamination: The main purpose of the process is to prevent wound infection, because all wound even meticulous sterile conditions are contaminated. The first W.B cells that reach the wound are the polymorphonuclear leukocytes, which start the phagocytosis process by fixing bacteria & digesting the invaders. Then macrophages = scavenger cells will reach the wound to engulf bacteria and neurotic tissue, even in poorly nourished tissues with low 02 level. Plus the scavenger job of the macrophages, it has another job (recruit fibroblasts). Fibro - blasts (repair cells) will respond to the chemical signals coming from the macrophages.
B) Neovascularization = capillary canalization or vascularsprouting: Healing will not take place, unless new blood vessels are present to supply 02 and nourishment to the injured tissue (injured tissues till now have no blood due to sealing off blood vessels & lymphatic). Patent vessels in the wound periphery develop small buds or sprouts that grow into the wound area. These outgrowths will eventually come in contact with other arteriolar or venular buds to from a capillary loop. These new capillary loops will fill the wound & erecting a red colour throughout the wound. Immobilization is essential during this phase to permit vascular regrowth and prevent new micro-hemorrhages. So early mobilization during this phase is contraindicated as well as heat application as the early shoulder motion in the inflammatory phase following mastectomy will lead to serous collection, wound breakdown and infection.
Heat application during this phase will increase bleeding from these fragile vessels. Lymphatic channels reopened to assist in decreasing wound edema. In normal condition, all these events of the inflammatory phase happen within the first 4 days after injury, unless there are complications that will increase the period more than 4 days. So during this inflammatory phase our aim is to decrease factors which prevent or prolong inflammationvia assisting the role of the macrophage scavenger cells through: the use of antibiotics, Debridment techniques (debris removing, proper positioning, RICE regimen, Low-dosage, pulsed ultrasonic in water baths will decrease infection and whirlpool cleaning.
2- Fibroblastic phase: rebuilding phase: With the inflammatory phase completed, rebuilding can commence (start or begin).The name of this phase is acquired from the repair cells or the cells of scar production (fibroblasts). The purpose of this phase is to repair or rebuild and to provide strength to the wound. Fibroblasts begin to synthesize or produce collagen. 3 Processes are included under the umbrella of the Fibroblastic phase to achieve wound closure: (1 st) Epithelialization. (2nd) Wound contraction. (3rd) collagen production.
A) Epithelialization: Epidermis of the skin has a stratified squamous epithelium (from the cell layers to the superficial cell layers). So epithelialization means =epidermal regeneration or surface covering. Within hours after injury, the undamaged epithelial cells (cells of epidermis) at the wound margin begin to reproduce epidermal regeneration or epithelial mitosis. These undamaged epithelial cells will migratory from the periphery toward the center of he wound cavity. These migratory cells remain attached to their parent cells, therefore, their movement will create a (pull) on the normal skin around the wound edge. Escher (scab = slough)from a temporary barrier for the wound and this Escher or scab must not be disturbed until epithelialization is complete. Escher will be attached to the wound and to the epithelial edge which dive downward to maintain contact with the vascular loop network.
Epithelial edges or margins will release lyric enzymes, which act cleave the attachments of the nonviable tissue as scab from the viable wound bed. With the completion of epithelialization slough or scab will be detached from the wound. In case of extensive wounds or with low 02, epithelial migration cannot be implemented. Epithelialization start with one thin layer just to cover the wound, and after several weeks epithelialization become multilayered including all epidermal layers, except basal layers leading to thin epithelialization. so epithelialization close the wound surface only not the deep.
B) Wound Contraction: Epithelialization close the wound surface only while wound contraction is a process, which pulls the whole, wound together leading to wound shrinking or decreasing the wound area. This wound contraction = wound shrinking and its centripetal force can useful in some regions and can be harmful and detrimental in other regions. If contraction is uncontrolled as in abdomen and gluteal regionwhere skin is loose and mobile, while the deep structures are fixed. In this condition wound contraction is useful with no contractors formation.
While in the hand region where joints, muscles, tendons and sheathes are very close to each other, So they are in need of every millimeter of skin & tissue length, so if wound contraction in hand is not controlled will create its centripetal force which pull all structures toward the wound leading to joint contractors as in cases of full-thickness hand burn, wound contraction and its centripetal force caused by specialized fibroblasts called the myofibroblasts.Difference between fibroblasts and the specialized myofibroblasts are that myofibroblasts contain the contractile properties of the smooth muscle cells.
Picture frame theorythe myofibroblasts (contractile fibroblasts): ring of the contractile fibroblasts (myofibroblasts) convene or accumulate near the wound perimeter forming a picture frame which will move inward toward the wound center to decrease the wound size. (N.B) wound contraction must be inhibited in hand burns & wounds. Skin graft will decrease wound contraction, however the thickness of the graft correlate with the degree to which wound or burn contraction is inhibited: • Split- thickness graft will decrease contraction of the wound bed by 31%
Full - thickness graft will decrease contraction by 55% • Full - thickness graft with splinting decrease contraction by 77%, So there is a negative correlation as increasing skin graft thickness will decreasing contraction. Grafting must beapplied early in the inflammatory phase before the beginning of wound contraction, but if grafting is applied Later on when the myofibroblasts are already mobilized and functioning, then excision of the wound margins (pictureframe) is essential before the application of skin grafting to prevent contraction from occurring under the graft.
C) Collagen production = glue production: wound healing occurs with collagen production, if there is no collagen production, no wound healing will be occurred. Migratory fibroblasts are now present throughout the wound and are stimulated to from & secrete collagen. Fibroblasts & collagen formation are need of adequate 02 supply .Fibroblast produces 3 polypeptide chains, These chains coil to from helix, these spiral chains called pro-collagen. Once pro-collagen is going out from the fibroblast to the extra - cellular space will be cleaved or divided at specific terminal sites, giving a triple helical molecule called the tropo-collagen molecule. The combination of the Tropo-collagen molecules together, will give collagen filament.
The aggregation (combination) of collagen filaments together, give collagen fibril. Aggregation of collagen fibril gives collagen fiber. Collagen fibers will accumulate in the wound in an irregular or disorganized manner and still in gelatinous state. Wound durability or tensile strength is dependent on the microscopic welding between collagen filaments. These sites of bonding or welding are called cross - links.
Welding or boning of the 3 chains together at the procollagen stage is still weak (Via hydrogen bonds) so vibration or heart application can denature and separate the chains of procollagen. With farther maturation into Tropo-collagen, the chains will develop a stronger cross-links which enhance stability but is not strong enough, these cross-links occurs within a single trop collagen molecule. Then with further maturation, cross - links will be developed between the tropo-collagen (from one tropo-collagen molecule to another molecule).positive correlation =increase number of links .increase tensile strength = or the wound durability.
The highest ratio the intermolecular bonds or the cross links is present in the bone tissue. Collagen can be presented as solution as well as rigid collagen gel, the only difference between the collagen solution & the rigid collagen gel is the number of bonds or cross - links. The wound at the end of this 3 weeks time, has the greatest mass of collagen but the tensile strength or the wound durability is still low. (only about 15 % of normal with a bulky, rough, tender red scar is visible & palpable).
3) Remodeling phase: Successful wound healing requires more than closing the wound with sufficient tensile strength. Remodeling requires the scar to change to fit the tissue. Remodeling of the scar maturation represent the final aggregation. Orientation and arrangement of the collagen fibers. 2 Processes are involved under the umbrella of the remodeling phase: • Synthesis - lysis balance: • Collagen fiber orientation
A)Synthesis lysis balance: Means the balance between the new collagen production process and the break down process of old collagen .New collagen formation = old collagen breakdown (under normal condition). If collagen formation is higher than old collagen breakdown this will lead to hypertrophic scar & Keloid formation. Collagen destruction or breakdown is occurred by the action of the collegians enzyme. Collegians enzyme is capable of cleaving strong cross-links or of the tropo- collagen molecule. Breaking these bonds causes the molecule to become soluble and excreted from the body as waste products.
Synthesis (New collagen production) is oxygen dependent while lysis (old collagen destruction) is oxygen independent. When balance between the 2 processes is abnormal as in cases of hypertrophic scars or keloid formation where normal synthesis is associated with lysis inhibition -» How we can restore balance and decrease the keloid formation? By the application of pressure (garments) to the scars, where prolonged pressure will lead to an ischemic condition with low O2 tension so synthesis is depressed (synthesis is O2 dependent), while lysis is continuous. Eventually, balance is achieved when the scar bulk is flattened to approximate normal tissue. Pressure therapy must be continued until remodeling is complete and all colognes return to the normal level, synthesis -lysis balance continues until remodeling phase ends at six months) to one year post injury (may be 2 years).
B) Collagen fiber orientation = collagen realignment: 2 theories are given to explain the forces which induce the collagen orientation process = collagen realignment; (1) The induction theory (2) tension theory. (1) The induction theory Tissue structure induce the collagen weave, then the scar attempts to mimic the characteristic of this tissue, dense tissues induce the formation of a dense, highly cross-linked scar(collagen). pliable (flexible) tissues induce the formation of a loose less cross linked scar, using the principles (inherent principles) of the induction theory, surgeon attempts to design the repair field by separating the dense from the soft tissues.
(2) The tension theory of collagen orientation: Tension theory reforest the internal & external stresses which affect the wound area during the remodeling phase, muscle tension, joint movement, splitting, temperature changes and mobilization are examples of forces acting on the collagen array. Scar stretching achieve only a temporary lengthening, but permanent elongation of the scar requires the stress (stretching) application for long-duration. Dynamic splints, stretching techniques and functional electrical stimulation (FES) are examples of methods used to achieve the low load long duration stress necessary to change scar configuration.
Negative effects of prolonged bed recumbency and the role of physical therapy: Just as training results in improvement in physical working capacity, inactivity leads to derogation. Until quite recently treatment for cardiothoracic and postoperative patient involved prolonged bed rest. However, the forced inactivity resulted in additional difficulties that were sometimes worse than the original problem.
Bed rest is anatomically and physiologically unsound, look at a patient lying long in bed. What apathetic picture he makes? The blood clotting in his veins, the lime draining from his bones, scybala stacking up in his colon, the flesh rotting from his seat, the urine leaking from his distended bladder, and the spirit evaporating from his soul. Get people up and we may save our patients from an early grave (death) and this is the role of physical therapy.
The effects of prolonged bed rest are reversiblewith adequate ambulating. The physiological effects, if not too advanced, can be reversible with an appropriate training program, a major problem is that the negative effects of bed rest lead to a vicious circle especially in the elderly: Disuse leads to debilitation, which leads to further desire to stay in bed or remain inactive. Psychologists have described bed rest as a from of sensory deprivation. Bad rest produces a greater incidence of intellectual inefficiency, bizarre thoughts exaggerated emotional reactions, time distortions, changes in body image, unusual body sensations, and an array of physical discomforts. As researchers put it. it may be better to burn out than to rust out
It has been concluded that, the most profound changes from bed rest occur in the cardiovascular system. Impairments include diminished capacity of the heart, reduced plasma & blood volume, and impaired automatically of the blood vessels.
Effects of the prolonged bed rest will decreases the following physiological functions: Red blood cell production Red cell mass Hemoglobin Serum albumin Serum proteins Bone calcium & density Insulin sensitivity Blood flow to extremities Muscular tone to extremities Systolic blood pressure Leukocyte phagocytic function and resistance to infection Delay wound healing. • Maximum stroke volume • Intracellular fluid volume • Plasma volume • Coronary blood flow • Pulmonary capillary blood flow • Skin blood flow • Arterial vasomotor tone • Cerebrovascular tone • Systolic time interval • Maximal 02 consumption • Balance • Orthostatic
Also effects of the prolonged bed rest will increases the following physiological functions: • Maximum heart rate • Diastolic blood pressure • Resting Heart rate • Extravascular & Intravascular immunoglobulin • Submaximal exercise Heart rate • Submaximal exercise Cardiac output • Diuresis • Sleep disturbances • Incidence of urinary infection • Incidence of DVT. • Urinary excretion of calcium & phosphorus • Nitogren excretion • Serum corticosteroids • Extracellular fluid • Tendency to faint & orthostatic intolerance • Incidence of constipation • Cholesterol • Low-density lipoproteins • Growth hormone • ST-segment depression in ECG
Also there are another postoperative complication as wound infections, respiratory problems, pressure sores, and the postoperative pain. These post operative complications plus the previously mentioned negative effects of the prolonged bed recumbency on the physiological functions can be prevented or at least minimized by a proper physical therapy program. It must be done preoperatively for patient education which helps greatly in application. The preoperative patient education must be done for one or more sessions to prepare patient for surgery and determining the post operative expectations & treatment.