Download
1 / 23
230 likes | 384 Views
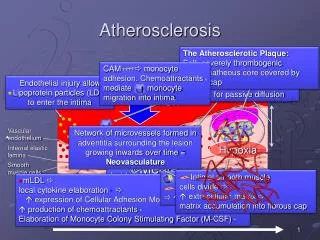
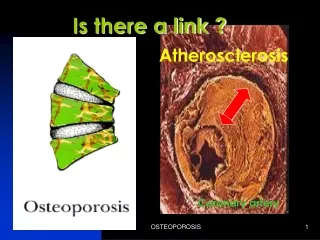
INTIMA MEDIA THICKNESS AND ATHEROSCLEROSIS. Michele CAZAUBON , MD, PhD American Hospital of Paris ( France) . INTIMA MEDIA THICKNESS AND ATHEROSCLEROSIS. ATHEROSCLEROSIS = ARTERIAL WALL DISEASE CLINICAL MANIFESTATIONS WHEN ADVANCED IMPORTANCE OF SCREENING FOR PRECLINICAL STAGE.

E N D
INTIMA MEDIA THICKNESS AND ATHEROSCLEROSIS Michele CAZAUBON,MD, PhD American Hospital of Paris ( France)
INTIMA MEDIA THICKNESS AND ATHEROSCLEROSIS ATHEROSCLEROSIS = ARTERIAL WALL DISEASE CLINICAL MANIFESTATIONS WHEN ADVANCED IMPORTANCE OF SCREENING FOR PRECLINICAL STAGE
DOPPLER ULTRASOUND IMAGING AND ARTERIAL WALL • PLAQUE • GRADE % • ECHOGENICITY INTIMA-MEDIA THICKNESS (IMT)
ANATOMICAL AND HISTOLOGY STUDY NORMAL ARTERIAL WALL IN B.MODE ULTRASOUND • • 1st ECHOGENIC LINEA = • LUMEN/INTIMA INTERFACE • 2nd ECHOGENIC LINEA = • / MEDIAL / ADVENTITIAL • PIGNOLI ( Circulation 1986)
IMT& ATHEROSCLEROSIS E= IMT D = DIAMETER Nb = NB OF Points 212/1cm
NORMAL VALUES IMT • 0,36 mm TO 0, 90mm = NORMAL VALUE IMT FOR ADULTS • AT THE SAME AGE : IMT > MEN / WOMEN • LINEARLY WITH AGE :0,08 mm/year • (SALONEN AND SALONEN ATHEROSCLEROSIS 1990 )
FEASABILITY OF MEASURE • 1/ CAROTID ARTERY • DISTAL COMMON CAROTID = 99% > BIFURCATION AND INTERNAL CAROTID
IMT AND « CLASSICAL » RISK FACTORS AGE GENDER SMOKING HIGH BLOOD PRESSURE CHLOL AND DIABETE
NEW RISK FACTORS /1 1 1/HYPERHOMOCYSTEINEMIA ASAP ( Antioxidant Supplementation inAtherosclerosis Prevention study ) -EIM dans groupe avec HC (SALONEN ANN MED INT 1998)
NEW RISK FACTORS /2 2/ STANDING AT WORK PROGRESSION = 0,08 to 0,67mm between men standing at work NEVER / ALWAYS. (SALONEN Environ Health 2000)
IMT& ATHEROSCLEROSIS NEW RISK FACTORS • 2/ STANDING AT WORK • « REDUCING THE DURATION OF STANDING AT WORK SHOULD BE CONSIDERED IN THE PRIMARY PREVENTION OF ATHEROSCLEROSIS » • (SALONEN Environ Health 2000)
IMT = SENSITIVE INDICATOR FOR THE PRESENCE OF PLAQUE IN THE BIFURCATION OF COMMON CAROTID EVA ’ STUDY ( Broussais .1996. 100 sujets 4 years follow up)
IMT c AND CAROTID STENOSIS CORRELATION BETWEEN IMT c AND SEVERITY ATHEROSCLERIS
ASSOCIATION BETWEEN IMT AND PREVALENCE OF PLAQUES BASELINE IMT - CCA IS AN INDEPENDANT PREDICTOR OF CAROTID PLAQUE OCCURRENCE INCREASED WALL THICKNESS PRECEDE PLAQUE FORMATION
IMT & CAROTIDATHEROSCLEROSIS • ROTTERDAM STUDY : • RISK ATHEROSCLEROTIC PLAQUES IN THE BIF CAR • X6 between IMT 0,63 mm / IMT 0,89 mm • (1996 . 7983 subjects population based study . GRADE B )
C IMT • • MYOCARDIAL INF. STROKE • 1/ INCLUSION = • 4476 SUBJETCS > 65 YEARS • WITHOUT CARDIO VASCULAR DISEASE • INCLUSION IMT measured : CC and Cint. • = 5 QUINTILES • 2/ FOLLOW UP = 6,2 YEARS • O ’LEARY et col. NEJM 1999 CARDIOVASCULAR HEALTH STUDY
RELATIVE RISK OF MYOCARDIAL INFARCTION AND STROKE / IMT ( first to fifth quintile) ___________________________________________________ IMT MI STROKE 1Q-5Q b a b a ------------------------------------------------------------------------ CC 4,50 2,46 3,86 2,13 ------------------------------------------------------------------------ CI 4,84 3 3,66 2,35 ------------------------------------------------------------------------ CC+CI 6,30 3,61 4,57 2,57 ____________________________________________________ b= inajusted a= after adjusted for age , sex and other risk factor. O ’LEARY et col. NEJM 1999 CARDIOVASCULAR HEALTH STUDY
CONCLUSIONS OF THE STUDY INTIMA MEDIA THICKNESS OF CC AND IC STRONGLY ASSOCIATED WITH THE RISK OF MYOCARDIAL INFARCTION AND STROKE IN ASYMPTOMATIC OLDER ( > 65 years) ADULTS .
IMT AND CORONARY CCA AND ICA IMT ARE ASSOCIATED WITH EXISTING CORONARY HEART DISEASE
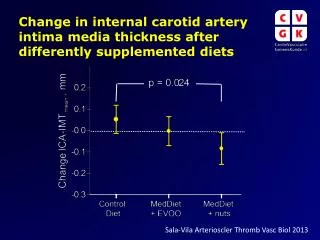
IMT AND THERAPEUTIC INTERVENTIONS LIPID LOWERING TREATMENT : STATINES +++ PRIMARY PREVENTION( ACAPS /CAIUS/KAPS) SECONDARY PREVENTION ( PLAC II/MARS/REGRESS) = REGRESSION OF PROGRESSION OF IMT BLOOD PRESSURES LOWERING DRUGS = DISCORDANCE HORMONE REPLACEMENT THERAPY = DISCORDANCE
MENOPAUSE/ IMT / AND CAROTID PLAQUES HORMONAL. NUMBER IMT c PLAQUES TREATMENT ( median value) HRT + 39 0,729mm 15% HR T - 55 0,782mm 51% HRT + = with hormonal replacement therapy HRT - = without hormonal replacement therapy p< 0,005 for IMT c and < 0,0001 for plaques M. CAZAUBON FA ALLAERT ANGEIOLOGIE 2001
CONCLUSIONS ULTRASOUND IMT MEASUREMENT = METHOD NON INVASIVE REPRODUCTIBLE NON EXPENSIVE FOR DETECTION OF EARLY ATHEROSCLEROSIS
CONCLUSIONS STRONG ASSOCIATION WITH VARIOUS RISK FACTORS FOR ATHEROSCLEROSIS ( classical and emergent) STRONG PRONOSTIC VALUE FOR CARDIOVASCULAR EVENTS = STROKE AND MYOCARDIAL INFARCTION IMT = GOOD MARKER FOR EFFICACITY OF ANTIATHEROGENIC DRUGS STRONG SENSIBILITY FOR STRATIFIACTION OF PETIENTS AT HIGH RISK FOR CARDIOVASCULAR DISEASE