Download
1 / 32
330 likes | 481 Views
Recent Risk Assessments Of Dioxins Comparing the WHO, COT, SCF and JECFA evaluations. J.C. Larsen (using many slides prepared by A.G. Renwick) Danish Institute of Food and Veterinary Research, Division of Toxicology and Risk Assessment, Mørkhøj Bygade 19, DK-2860 Søborg, Denmark.

E N D
Recent Risk Assessments Of Dioxins Comparing the WHO, COT, SCF and JECFA evaluations J.C. Larsen (using many slides prepared by A.G. Renwick) Danish Institute of Food and Veterinary Research, Division of Toxicology and Risk Assessment, Mørkhøj Bygade 19, DK-2860 Søborg, Denmark
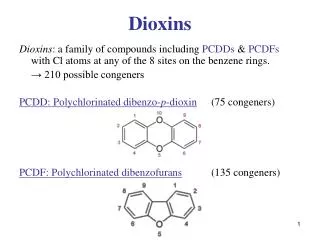
Polychlorinated dibenzodioxins Polychlorinated dibenzofurans Co-planar polychlorinated biphenyls
e.g. Fingerhut et al., 1991 Ott and Zober, 1996 Manz et al., 1991 Flesch-Janys et al., 1995 Becher et al., 1996 Coggon et al., 1991 Exposed workers Environmental Local accidental high exposures Differences in background low level exposures Seveso e.g. Bertazzi et al., 2001 Rotterdam and Groningen cohorts e.g. Huisman et al., 1995 Koopman-Esseboom et al., 1996 HAZARD IDENTIFICATION Human studies Epidemiology
Genetic Studies in bacteria and mammalian cells were generally negative, does not bind to DNA, not genotoxic Acute Oral LD50 is 1 - 5000mg/kg (guinea pig – hamster) Short-term Studies in mice rats, guinea pigs and monkeys; metabolic effects and changes in liver, thymus and haematology Long-term and carcinogenicity Decreased weight gain, increased mortality (F), splenic and thymic atrophy, hepatic degeneration plus increase in thyroid follicular and hepatic carcinomas in rats Reproductive Multi-generation studies – deceased fertility (rats) Single-generation studies – decreased sperm count (rats) Developmental studies – cleft palate and hydronephrosis (mice), effects on testes, prostate and sperm count (rats) HAZARD IDENTIFICATION (TCDD) In vitro and animal studies
HAZARD CHARACTERISATION 1. Selection of effects that are of relevance to humans 2. Identification of effect(s) produced at the lowest doses 3. Dose-response assessment of effects and consideration of mode of action (threshold or non-threshold) 4. Derivation of a health-based advice related to the risk associated with the critical effect(s) (threshold or non-threshold)
For Dioxins the effects are considered to be mediated via the AhR [or other threshold mechanisms] so that the usual NOAEL + uncertainty factor approach is suitable Recent studies with knockout mice show that the AhR is important in:- Effects on liver, thymus(?), epididymis, testes – Lin et al., 2001 Effects on prostate - Lin et al., 2002 Oxidative stress and vascular inflammation – Hennig et al., 2002 T-lymphocyte suppression – Kerkvliet et al., 2002 Keratinocyte differentiation – Loertscher et al., 2002 Are the extensive epidemiological data adequate for risk assessment? Are exposure data reliable - both quantitatively and in relation to confounding exposures? Does hazard characterisation in human studies include all hazards identified in animal studies?
Blood lipids – inconsistent changes Chloracne – no clear dose-response reported Cancer – largely based on occupational exposures Cardiovascular disease – inconsistent evidence Immunological effects – inconsistent findings Liver – increases in liver enzymes Neurological effects – inconsistent findings Neurodevelopmental – some differences in ongoing Dutch studies Reproductive hormones – inconsistent changes Reproductive outcomes – change in sex ratio (Serveso) Respiratory system – inconsistent evidence Thyroid function – small and inconsistent changes Urinary system – no major changes reported HAZARD CHARACTERISATION Human studies Based on COT, 2001
HAZARD CHARACTERISATION Animal studies Female Rhesus monkeys given 0.15 ng/kg bw/day in the diet for 3.5 years Schantz & Bowman (1989) - reported subtle, non-persistent neurobehavioural changes (object learning) in offspring (16.2 and 36.3 months). Rier et al (1993) – reported increased incidence of endometriosis after 10 years Mably et al (1992a,b,c) – reported decreased weights of epididymis and sperm numbers in rats after a single oral dose of 64ng/kg on gestation day 15 (GD15). Gray et al (1995, 1997a, 1997b) – reported greater effects on male offspring following single oral dosage on GD15 compared with GD8, with significant decreases in sperm count after 50ng/kg Faqi et al (1998) – reported effects on sperm production in offspring following 25ng/kg as a subcutaneous loading dose 2 weeks prior to mating followed by weekly maintenance doses of 5ng/kg Ohsako et al (2001) – reported decreased anogenital distance in offspring following 50ng/kg by gavage on GD15. NOAEL was 12.5 ng/kg bw.
Hazard Characterisation Rodents require higher doses (100-200-fold) to reach the same equivalent body burdens as seen in humans at background exposures. Body burden estimations are considered the most appropriate dosimetric parameter for interspecies comparison.
What intake in humans would give a maternal body burden of TCDD of for example 30ng/kg? TCDD would show slow accumulation on repeated daily intake, because the half-life of TCDD in humans is very long (7.5 years)
35 30 25 20 Body load (ng/kg) Body burden = daily intake x bioavailability x half-life 0.693 15 10 5 0 0 10 20 30 40 50 60 70 Time in years Daily intake = body burden x 0.693 bioavailability x half-life
35 30 25 20 Body load (ng/kg) 15 10 5 0 0 10 20 30 40 50 60 70 Time in years Daily intake = body burden x 0.693 bioavailability x half-life Daily intake = 30 ng/kg x 0.693 0.5 x 7.5 years Daily intake = 15 pg/kg/day
ANIMAL BODY BURDENS OF TCDD AND ASSOCIATED HUMAN ESTIMATED DAILY INTAKES (EDI)(WHO 1998)
Estimation of a TDI for dioxins (WHO 1998) The LOAELs for the most sensitive adverse responses in experimental animals could be transformed into arange of estimated long-term human daily intakes of 14-37 pg/kg bw/ day. Composite uncertainty factor of 10: TDI 1 - 4 TEQ pg/kg bw (rounded figures)
Limitations of the design of the rat studies used by WHO The bioavailability of 2,3,7,8-TCDD to the foetus is likely to be higher following a single oral bolus dose on days 15 - 16 of gestation (the sensitive window) than after low-level chronic dietary exposure at steady state.
HAZARD CHARACTERISATION Animal studies The key to the use of these data for risk assessment came with the studies of Hurst et al (2000a,b) who reported the tissue distribution of 3H in maternal and fetal tissue on GD16 after administration of [3H]-TCDD as a single dose on GD15 and following subchronic exposure (5 days per week for 13 weeks) Maternal Fetal Dose on GD 15 Dose on GD 15 Fetal Maternal Daily dose Daily dose
Single dose on GD15 Subchronic exposure Dose ng/kg Maternal ng/kg Fetal ng/kg Mat/Fet ratio Daily dose ng/kg Maternal ng/kg Fetal ng/kg Mat/Fet ratio 50 30 5.3 5.7 0.71 20 1.4 14.3 200 97 13.2 7.4 7.1 120 7.5 16.0 800 523 39.1 13.4 21.3 300 15.2 19.7 1000 585 55.7 10.5 HAZARD CHARACTERISATION Animal studies The key to the use of these data for risk assessment came with the studies of Hurst et al (2000a,b) who reported the tissue distribution of 3H in maternal and fetal tissue on GD16 after administration of [3H]-TCDD as a single dose on GD15 and following subchronic exposure (5 days per week for 13 weeks)
COT- used ratio of 2.5 based on the 2 lowest doses Single dose on GD15 Subchronic exposure Ratio Dose ng/kg Maternal ng/kg Fetal ng/kg Mat/Fet ratio Daily dose ng/kg Maternal ng/kg Fetal ng/kg Mat/Fet ratio 2.5 50 30 5.3 5.7 0.71 20 1.4 14.3 Correction Factor Applied SCF– fitted power functions to the data for the GD15 and subchronic data and derived a correction factor of 2.5 at maternal body burdens of <30ng/kg and 2.6 from 30-100ng/kg. The SCF established corresponding values of fetal, acute maternal and subchronic steady state maternal body burdens for 2,3,7,8-TCDD JECFA– fitted power functions to the data for the GD15 and subchronic data and derived a correction factor of 2.6; also fitted a linear model and estimated possible TDI values using each correction method
Selection of a NOAEL or LOAEL on which to base the TDI Faqi et al (1998) appear to have detected the most sensitive endpoints for which the LOAEL is 25ng/kg loading dose plus 5ng/kg every 7 days
Estimation of the maternal subchronic steady state body burden (BB) associated with the Faqi et al. (1998) LOAEL At GD 16 the maternal BB consisted of a (“pseudo”) steady state BB of 20 ng/kg bw and an acute BB of 5 ng/kg bw from the injected loading dose. Using the tabulated corresponding values of fetal, acute maternal and subchronic steady state maternal BBs the SCF estimated a fetal BB of 1.8 + 1.2 = 3.0 ng/kg bw. The 3.0 ng/kg bw fetal BB would correspond to a maternal subchronic steady state BB of 39 ng/kg bw.
Estimation of the daily intake in humans that would give the same maternal body burden Daily intake = 39 ng/kg x 0.693 0.5 x 7.5 years Daily intake = 20 pg/kg bw
Usually 3 or 10 No NOAEL only a LOAEL in critical study No chronic bioassay No developmental/repro’ toxicity data Uncertainty factors Database deficiencies
SPECIESDIFFERENCES HUMANVARIABILITY KINETICS DYNAMICS KINETICS DYNAMICS Usually 100 10 10 Uncertainty factors Inter-species extrapolation Inter-individual variability
100 - FOLD UNCERTAINTY FACTOR INTER-INDIVIDUAL INTER-SPECIES DIFFERENCES DIFFERENCES 10 - FOLD 10 - FOLD TOXICO- DYNAMIC ADUF 10 0.4 2.5 TOXICO- KINETIC AKUF 10 0.6 4.0 TOXICO- DYNAMIC HDUF 10 0.5 3.2 TOXICO- KINETIC HKUF 10 0.5 3.2 Chemical specific data can be used to replace a default uncertainty factor (UF) by an adjustment factor (AF) - based on IPCS 1999, 2001
Taken into account by calculation of maternal body burden TOXICO- DYNAMIC ADUF 10 0.4 2.5 TOXICO- KINETIC AKUF 10 0.6 4.0 TOXICO- DYNAMIC HDUF 10 0.5 3.2 TOXICO- KINETIC HKUF 10 0.5 3.2
Taken into account by calculation of maternal body burden Rats are more sensitive than humans and as sensitive as the most sensitive human TOXICO- DYNAMIC ADUF 10 0.4 2.5 TOXICO- KINETIC AKAF TCDD 1.0 TOXICO- DYNAMIC HDUF 10 0.5 3.2 TOXICO- KINETIC HKUF 10 0.5 3.2
No data available Taken into account by calculation of maternal body burden Humans are generally less sensitive than rats, but the most sensitive human might be as sensitive as rats TOXICO- DYNAMIC ADAF TCDD 1.0 TOXICO- KINETIC AKAF TCDD 1.0 TOXICO- DYNAMIC HDAF TCDD 1.0 TOXICO- KINETIC HKUF 10 0.5 3.2
Database deficiencies 3 9.6 Inter-species extrapolation 1 Inter-individual variability 3.2 Uncertainty factor for TCDD 20 pg/kg/day gives a maternal body burden of 39 ng/kg Dividing by the 9.6-fold uncertainty factor gives a daily intake of 2.1 pg/kg This was rounded to give a tolerable intake of 2pg/kg/day
Guidance values expressed as 2,3,7,8-TCDD equivalents WHO (1998) – gave a range of 1- 4 pg/kg/day – because intake data are usually expressed on a daily basis SCF (2001) – gave a value of 14pg/kg/week – to reflect the long half-life of TCDD JECFA (2002) – gave a value of 70pg/kg/month – to reflect the long half-life of TCDD Note – one day = 0.04% of the half-life – one week = 0.25% of the half-life – one month = 1.11% of the half-life Therefore – the main rationale of longer time intervals is to emphasise that short-term peaks of exposure will not greatly affect body burden - rather than indicate a duration of exposure that could affect body burden
Conclusions Recent evaluations by the COT, SCF and JECFA have been based on changes in the male rat reproductive system following in utero exposure • Conversion of the animal data into a tolerable intake for humans has allowed for • the fetal to maternal ratio after bolus dose • the long half-life and potential for accumulation • the relative sensitivity of rats and humans • potential human variability in kinetics and dynamics The COT, SCF and JECFA differ in the time-base of the guidance value but not in the data or approach used The intake by a significant proportion of the population exceeds the guidance value