Download
1 / 49
500 likes | 751 Views
NPSA Chemotherapy Project. Dermot Ball Chemotherapy Project Pharmacist dermot.ball@npsa.nhs.uk. Structure & function of the NPSA Chemotherapy Project Oral chemotherapy Treatment Plan BNF Chapter 8 Website. About the NPSA Arms length body of the Department of Health.

E N D
NPSA Chemotherapy Project Dermot Ball Chemotherapy Project Pharmacist dermot.ball@npsa.nhs.uk
Structure & function of the NPSA • Chemotherapy Project • Oral chemotherapy Treatment Plan • BNF Chapter 8 • Website
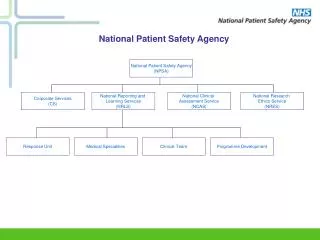
About the NPSAArms length body of the Department of Health • NRES- National Research Ethics Service provides safety and dignity of research participants by facilitating ethical research • NCAS- National Clinical Assessment Service provides confidential services to help manage concerns with the performance of practitioners • NRLS- National Reporting and Learning Service improves patient safety by enabling the NHS to learn from patient safety incidents
The journey so far An Organisation with a Memory(June 2000) ‘failures often have a familiar ring….strong similarities to incidents which have occurred before…almost exact replication’ Building a Safer NHS for Patients (May 2001) ‘A new independent body, the NPSA, will be established within the NHS’ Safety First (Dec 2006) ‘NRLS should identify sources of risk and harm…acted upon at a local and national level’
Size of the problem • ‘First do no harm’ or ‘to help, or at least do no harm’ (Hippocrates 4th Century BC) • Medical error accepted as part of practice • A study in the USA estimated that 44,000 to 98,000 die each year from medical mistakes1 • NHS hospitals – harm in about 10% admissions – in excess of 850,000 a year • £2 billion a year in additional hospital stays • £400 million a year in negligence claims 1 Brennan et al. (1991) New England Journal of Medicine 324:377-384
Patient Safety Incident (PSI) • A patient safety incident is an event or circumstance which could have resulted, or did result, in unnecessary harm to a patient. • An adverse event is an incident which results in harm to a patient.
Errors and violations • An error may be defined as a failure to carry out a planned action as intended or application of an incorrect plan. • A violation implies deliberate deviation from an operating procedure, standard or rule.
Incident vs Error • Cardiac arrest under general anaesthesia • Related to violations • About 75% of adverse events involve error
Contributing Factor • A circumstance, action or influence which is thought to play a part in the origin or development of an incident, or to increase the risk of an incident. e.g. distraction/inattention, fatigue/exhaustion, cognitive factors, communication, protocols/procedures, resources/workload.
Part of clinical governance • "A framework through which NHS organisations are accountable for continually improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish." G Scally and L J Donaldson, 'Clinical governance and the drive for quality improvement in the new NHS in England' BMJ (4 July 1998): 61-65
Part of quality Effectiveness Efficiency Safety Appropriateness Patient-centred Access
Nothing new - 400 years ago -“Cure the disease and kill the patient” Francis Bacon (1561-1626) - 300 years ago -“Cur’d yesterday of my disease, I died last night of my physician” Matthew Prior (1664-1721) -200 years ago -“I do not want two diseases - one nature-made, one doctor made” Napoleon Bonaparte (1769-1821)
Patient Safety Is Important Safer Care not just a by-product of well educated, well intentioned staff - needs to be ‘hardwired’ into the design and delivery of systems of care….. • Unsafe Caresignificant source of patient morbidity and mortality - major cause of distress to patients and families we need safe individuals and safe systems
The Role of the NPSA and the Reporting and Learning System capture and analyse incidents learn from mistakes change practice & system factors to reduce risk improve patient safety in the NHS
NPSA philosophy • learn from things that go wrong • improve patient safety in frontline services • systems not individuals • learning not judgement • fairness not blame • openness not secrecy • develop and implement solutions to problems
Incident Reporting • Adapted from the critical incident technique in aviation • Relies on good safety culture • Inherent value is in the learning • Near misses collected • Should not be used for epidemiological analysis • Under-reporting will always occur
Reporting Routes Local paper form Specifics e.g. HSE, MHRA FRONTLINE STAFF RISK TEAM SHAs or WAG (SUIs) Local eform RLS NPSA eform Patient
Analysis tools Data Cleansing RLS Database Reports & Analysis Reporting to NPSA 99% upload from local trust reporting system eform
NRLS RLS Database Database Outputs
Quarterly Reports Trends in reporting and profile of reports Clinical topics in each issue such as: Chemotherapy Project Available on website
Thematic Analysis 424/576 deaths reported to the NRLS in 2005/06 occurred in acute hospitals 3 key themes: Diagnostic errors (n = 71) Clinical deterioration not recognised or not acted upon (n = 64) Problems with resuscitation after cardiopulmonary arrest (n = 43 in acute/general hospitals)
2000 Systematic review of RLS death & severe incidents Systematic review of STEIS reports Ad hoc incident / issue reports e.g. coroners, clinicians 50 Incidents & issues considered by the Weekly Response Group ESTIMATE OF INCIDENTS AND ISSUES FLOWING THROUGH RESPONSE UNIT PER MONTH 20 Issues followed up with mini-scope e.g. RLS search, basic literature search 4 Full-scope 1
Acting on Urgent Risks • Fast-track urgent issues identifies immediate action • System to track activity with deadline • Evaluation shows support for one-pager • Oral chemotherapy • Vinca Alkaloids
Adapted from REASON, 2005 Organisation Environment Workspace Factors within the healthcare system that could potentially lead to harm Task The ‘system’ Equipment People Staff act as harm absorbers • Staff Patients
Cancer Projects • Radiotherapy • Chemotherapy • Early Diagnosis
Chemotherapy Project • Between Nov 2003 and June 2008 • 219,000 patient safety reports (medication) • 4829 (2.2%) anti-cancer medicines • Manual validation 25/272 • 8 Deaths, 9 Severe Harm, 8 Moderate Harm • 6 deaths associated with ORAL CHEMOTHERAPY • >95% resulted in Low Harm or No Harm
Chemotherapy Project • 43% of errors associated with administration • 33% of errors associated with wrong dose, frequency or quantity of medication • 18% of errors associated with delayed or omitted treatment
Chemotherapy Project • Taxanes – 436 reports • Cisplatin – 404 reports • Etoposide – 396 reports • Capecitabine – 368 reports • Cyclophosphamide – 359 reports • 35 named drugs
Chemotherapy Project • Quantitative data - limitations • Qualitative data - limitations • Eight emerging themes • Trends • 20 recommendations • Links to NCEPOD, NCAG
Data often incomplete No specific research question Exaggeration of degree of ACTUAL harm Potential harm not easy to assess Large amounts of ‘noise’ Side effects, ADR, extravasation, protocols followed correctly Chemotherapy Project
An F2 doctor was electronically prescribing chemotherapy whilst his consultant, oncology pharmacist and System Administrator were away on annual leave. • The patient’s serum creatinine was not automatically entered on the system, so the doctor attempted to do it manually. • The level was entered incorrectly and a low creatinine clearance was subsequently produced. • This resulted in a low dose of carboplatin being calculated, which the doctor amended manually by changing the AUC to 30.1 resulting in a 500% dose increase. • Three weeks later a second unsupervised F2 doctor, again working without Consultant supervision prescribed further carboplatin for the same patient. The dose of 4875mg was queried by the pharmacist and reduced(!)
A patient had been changed from OxMdG to capecitabine and oxaliplatin. The nurse selected the OxyCap regimen from the computer, and they received their first cycle. On returning for their second cycle it was realised they should have received XelOx. On the computer OxyCap referred to an arm of FOCUS 2 which delivered a 30% dose reduction of the two drugs. • A patient was receiving ifosfamide and Mesna and three doses of Mesna were omitted resulting in the patient experiencing haemorrhagic cystitis.
A 69 year-old patient with relapsed multiple myeloma received four times the intended dose of idarubicin. He was admitted with neutropenic sepsis from which he did not recover and he died 11 days after commencing the idarubicin. • In the process of completing an SAE form following the sudden death of a patient, it was noticed that he had received four cycles of capecitabine at 1250mg/m2. As the patient was >70 yrs the QUASAR TT protocol indicates that his maximum dose should have been 1000mg/m2. • A chemotherapy trial patient was admitted due to acute breathlessness. Scans had shown pulmonary fibrosis, pulmonary emboli and a pleural effusion. He died in ITU 6 days later of pulmonary fibrosis secondary to receiving an overdose of bleomycin - on seven separate occasions.
A patient had received two prior cycles of PECC for relapsed NHL • Prednisolone 40mg daily for 7/7 days • Etoposide 400mg daily for 3/7 days • Chlorambucil 40mg daily 4/7 • CCNU 200mg daily 1/7 • For his third cycle the prescription was misread and he received • Etoposide 400mg daily for 8 days • CCNU 200mg daily for 7 days • Prednisolone & Chlorambucil were correctly supplied • The patient’s concerns regarding the extra medication were ignored • He was admitted 10 days after starting 3rd cycle with toxicity • He died 30 days after admission as a result of the excessive doses
BNF Chapter Eight • “A little knowledge is a dangerous thing” • Long standing concern regarding the advice it offers and how it’s interpreted • Doesn’t fully reflect the complexities of current chemotherapy, especially oral treatments • Lack of consistency re; dosing information • Status of BNF “brand” may provide a false sense of security for non-specialists • Cancer professionals use other sources
BNF Chapter Eight • “Be very afraid……” • Main focus is introductory section • Standardisation of drug monographs? • BNF acknowledge that some changes may be required • Draft chapter for consultation • BNF editorial policy • Oncology Pharma input?
Treatment Plan • Open to interpretation! • Is it a Protocol – no • Is it a Patient Diary – no • Is it something in between – probably!
Not designed as patient information Not part of the Information Prescription project Target audience is primarily non-specialists Patient is the ‘conduit’ Potentially valuable during any health care intervention; Admission Discharge Dispensing Reviewing Treatment Plan
Web-based support • Cancer Network websites as a resource for (oral) chemotherapy safety? • 30 Networks, ~ 5 have readily accessible information on chemotherapy protocols • Web site quality extremely variable! • NPSA to develop a standard template with North of England Cancer Network • To be continued…….
Summary Patient Safety is part of NHS care Incident reporting is the key to learning Admitting failure is the sign of a mature organisation Learning needs to take place at local and national level Cancer patients can benefit from patient safety initiatives