Download
1 / 28
350 likes | 738 Views
A conceptual framework for Project MAMI (Management of Acute Malnutrition in Infants 0-5.9m). Towards a common understanding of the causes and classification of infant malnutrition. NB. DRAFT!!!. THANK YOU FOR COMMENTS / FEEDBACK!!!. AIM. To investigate the management of

E N D
A conceptual framework for Project MAMI(Management of Acute Malnutrition in Infants 0-5.9m) Towards a common understanding of the causes and classification of infant malnutrition
NB. DRAFT!!! • THANK YOU FOR COMMENTS / FEEDBACK!!!
AIM To investigate the management of acutely (moderately and severely) malnourished infants under six months age (0-5.9m) in emergency programmes, in order to establish consensus on (interim) good practice guidelines: ‘DOABLE’ EVIDENCE BASED INDIVIDUAL(CLINICAL) vs PUBLIC HEALTH
To discuss • What do we mean by “malnutrition” (10mins) • Conceptual framework for causes of acute malnutrition in infants 0-5.9m (10mins) • Way forward for MAMI: (10mins) • FOCUS: What do you need from the project • SCOPE: What data is available what is realistic to do within the timeframe • OUTPUTS: What like to see • OTHER….
Why does MAMI need a conceptual framework? • Classification of malnutrition in infants 0-5.9m is not simple • Preventative as well as curative interventions are vital for the ‘management’ of acute malnutrition • Developing a common understanding of: • What causes are • How to classify cases is therefore important as we start the project JOINT UNDERSTANDING BETTER COMMUNICATION (internal AND external…)
1st: What do we mean by ‘Malnutrition’A (DRAFT) Working Classification ?? (how) can we distinguish?? MAMI
(DRAFT) Expanded Framework for 0-5.9m ?constitutional? INADEQUATE INTAKE + INADEQUATE ACCESS • Disease • Acute - infection • BMS related • (pneumo, GE, sepsis) • Malabsorbtion • Chronic - Syndrome (Downs, other) • - Metabolic • - congenital infection. • treatable – e.g. syphilis • ??treatable-CMV, rubella • - HIV • - TB B) NOT CURRENTLY EBF (BMS =whole/part of diet A) CURRENTLY ‘EBF’ MAMI
(DRAFT) Expanded Framework for 0-5.9m ?constitutional? • INADEQUATE CARE • 1) Reduced time for infant feeding • economic factors • - employment law / conditions • 2)BF ‘Environment’ difficult • - cultural / employment / religious issues • 3) Orphans • 4) Myths & Misconceptions INSUFFICIENT HEALTH SERVICES & UNHEALTHY ENVIRONMENT 1)Myths & misconceptions -’stress’ & BF 2)TREATABLE disease not adequately treated 3)Inadequate clean water (quality; quality) MAMI
(DRAFT) Expanded Framework for 0-5.9m ?constitutional? INADEQUATE INTAKE + INADEQUATE ACCESS • Disease • Acute - infection • BMS related • (pneumo, GE, sepsis) • Malabsorbtion • Chronic - Syndrome (Downs, other) • - Metabolic • - congenital infection. • treatable – e.g. syphilis • ??treatable-CMV, rubella • - HIV • - TB B) NOT CURRENTLY EBF - Inadequate quantity of BMS (formula/other milk/ solid food) - Inadequate quality of BMS - inappropriate dilution - inappropriate BMS - inadequate equipment - inadequate fuel a) No chance resume BF -orphan, no wetnurse ib Possibility to resume BF - HIV related choice Frequent pregnancy • A) CURRENTLY EBF • i) Suboptimal BF performance: • a) Infant reasons • - ‘skills’ e.g. dev. delay/CP -- illness (acute) • - Congenital problem • - e.g cleft palate • b) Maternal reasons: • Skills • Lack of emotional support • Psychological (clinical depression) • Severe maternal malnutrition (macronuts) • Severe maternal malnutrition (micronuts) • ii)Ex premature inf • - increased micronut needs • INADEQUATE CARE • 1) Reduced time for infant feeding • economic factors • - employment law/conditions • 2)BF ‘Environment’ difficult • - cultural / employment / religious issues • 3) Orphans • 4) Myths & Misconceptions INSUFFICIENT HEALTH SERVICES & UNHEALTHY ENVIRONMENT 1)Myths & misconceptions -’stress’ & BF 2)TREATABLE disease not adequately treated 3)Inadequate clean water (quality; quality) MAMI
Other Aspects - Critical but outside project scope Factors to note: MAMI
WAY FORWARD • FOCUS: What do you need from the project? • SCOPE: What data is available? What is realistic to do within the timeframe? • OUTPUTS: What would you like to see? • OTHER….
Invitation to Collaborate Please help us develop the evidence base to improve the management of malnourished young infants Project websites: http://www.ucl.ac.uk/cihd/research/nutrition/mami http://www.ennonline.net/ife/ Contact: Marko Kerac Email: marko.kerac@gmail.comom
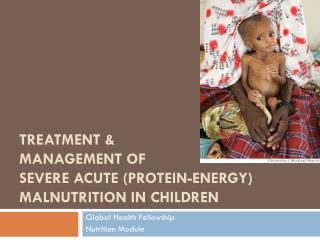
MAMI(Management of Acute Malnutrition in Infants)Funded by UNICEF-led IASC Nutrition Cluster A retrospective review of the current field management of acutely malnourished infants under 6 months of age http://www.ucl.ac.uk/cihd/research/nutrition/mami
AIM To investigate the management of acutely (moderately and severely) malnourished infants under six months age (0-5.9m) in emergency programmes, in order to establish consensus on (interim) good practice guidelines
Objectives • To establish what currently is advised or recommended in the form of guidelines, policies and strategies by different organisations. Particularly to consider: - admission and discharge criteria - therapeutic management - care practices & psychosocial support - breastfeeding support
Objectives • To determine what is carried out in practice - are policies reflected by practice? - numbers and % of TFP/SFP admissions 0-5.9m age - numbers admitted vs numbers expected (DHS surveys) (proxy measures of coverage) • To examine current outcomes for 0 – 5.9m infants - what affects outcomes? - key contextual factors (modifablevs non-modifiable) - what are key challenges and constraints?
Collaboration TO BE OF PRACTICAL RELEVANCE TO FIELD-BASED PROGRAMMES: We need your inputs NOW… *** INVITATION TO COLLABORATE *** The closer our collaboration… The better & more useful the final outputs… Interagency Steering Group Research Advisory Group
Background • Very few formal research studies investigating acute malnutrition in infants 0- 5.9 months of age Poor evidence base upon which to base field guidance materials Difficult to know how best to support these infants in practice Many current malnutrition strategies do not specifically address the needs of this age group
Background • Over 6 years of published concerns, documented field experiences and debate by ENN and by the IFE Core Group • WHO Technical review of the Management of Severe Acute Malnutrition (2004): “ No new research was identified pertaining to the optimum dietary management of severely malnourished infants aged < 6 months. The evidence base for defining the most advantageous formulations for feeding this age group remains weak ”
Field Reality • Young infants still present to field based programmes ! • Variable capacity and skills to manage them: • Some programmes good we need to learn from them • Some ‘could be better’ • Lactating women with infants 0-5.9 months may be admitted to Supplementary Feeding Programmes (SFPs), But… • No standard guidance on the breastfeeding & infant feeding support that should form part of the package of care.
Field Reality & Field Evidence • Operational agencies undertake different types of intervention sometimes guided by applied / operational research. field experience is growing / significant… But… • Field evidence too often hidden… • Programme data collected but not formally analysed • Internal reports written but not routinely disseminated / shared
Why field evidence is vital • ‘Background’ for changes in official guidance (WHO) • Knowing about current field practices helps inform, target, and manage change • Stronger understanding of ‘who does what, where’ for MAMI directly facilitates future collaborations and research • Project ownership • Collaborations and partnerships during the review process project more focused, more relevant to field organizations • Shared project ownership guidelines & recommendations more likely to be taken up
Planned Project Outputs • (Interim) ‘Best Practice’ guidelines ~ Based on best currently available evidence ~ Explicit about underlying evidence (or lack of) for each step • Research Agenda ~ Understanding of gap areas can suggest specific studies • Bigger IYCF picture ~ Consider management strategy in the context of IYCF recommendations for general population • Strengthened organizational linkages / ongoing collaborative efforts ~ Supporting guideline implementation ~ Facilitating new or ongoing research / operational research
Results Dissemination • ENN Special Supplement • Peer reviewed paper(s) • International fora: • IASC Nutrition Cluster meetings • UN SCN meeting in 2009 • Inputs into review / update of WHO guidance for Management of Acute Malnutrition
Some contextual issues • The rise of CMAM (CTC) • What place for young infants within current CMAM contexts? • What place for young infants in future projects? • Rollout of new WHO standards • Numbers diagnosed with SAM/MAM differ if NCHS references vs new WHO standards % of median vs Z-score Understand likely effects of change in diagnostic criteria
Other issues to discuss.. • ? Disaggregateage groups (0-1.9m, 2-3.9m, 4-5.9m) • ? ‘malnutrition’ aetiology: • ex-premature infants; LBW infants; postnatal growth failure alone • ? Infants older than six months but less than 4kg • ? HIV related issues • ‘rapid weaning’ of breastfed infants at ~6 months of age • ? Focus on NGO programmes (?context of other services/providers) • ? Other YOUR inputs /ideas / comments are CRITICAL…
Please get involved… *** ‘INVITATION TO COLLABORATE’ document *** ** Special session MAMI WEDNESDAY 7pm ** * email: marko.kerac@gmail.com *