Download
1 / 61
690 likes | 779 Views
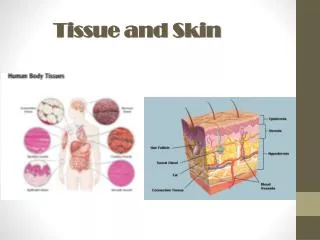
SSTI skin and soft tissue infection. By :Dr. Sha`bani. Anatomy of the Skin. Epiderm is devoid of blood vessels then disruption of it allows penetration of bacteria to deeper layers The hair follicle can serve as a portal

E N D
SSTIskin and soft tissue infection By :Dr. Sha`bani
Epiderm is devoid of blood vessels then disruption of it allows penetration of bacteria to deeper layers • The hair follicle can serve as a portal • Intracellular infection of the squamous epithelium with vesicle formation arise from: 1-cutaneous inoculation(HSV-1) 2-dermal capillary plexus( varicella and other viremia) 3-cutaneous nerve root( herpes zoster)
Infective vasculitis of plexus capillary beneath the dermal papillae results in petechia, osler node, janeway, and palpable purpura • Exaggeration of these physiologic mechanisms by excessive level of cytokines or bacterial toxins causes leukostasis ,venous occlusion and pitting edema. Edema with bullae ,ecchymosis and anesthesia suggest loss of vascular integrity and should be evaluated for nec. Fasc. Or myonecrosis
CRUSTED LESIONS • Impetigo • Superficial dermatophyte infection • Infection with dimorphic fungi( sporothrix) • Crusted nodular infection ( mycobacterium chelonei)
Impetigo • initially vesicular, later crusted • superficial • group A streptococcus and Staphylococcus aureus( the sec. is more common) • Non-bollous and bollous • On exposed area • The purulent discharge dries and forms the characteristic thick, golden-yellow, “stuck-on” crusts. • mild regional lymphadenopathy • Healing without scarring • constitutional manifestations are minimal
Differential Diagnosis. • Varicella, the crusts of impetigo are darker brown and harder • When the vesicles of herpes simplex become turbid, they may resemble those of impetigo. • Localized acute pustularpsoriasis may also be mistaken for impetigo. • Atopic or contact dermatitis, discoid lupus erythematosus, and infestations such as scabies may mimic impetigo or develop secondary impetiginization
Treatment • Penicillinase-resistant oral penicillins (e.g., dicloxacillin or amoxicillin-clavulanate) or cephalosporins (e.g., cephalexin) • Erythromycin or newer macrolides for β-lactam–allergic patients • TMP/SMX – clindamycin- • Topical antibiotic therapy may be considered when treating limited impetigo ,including that caused by MRSA.(mupirocin ointment- fusidic acid
Bullous Impetigo • neonates and young children • begin as vesicles that turn into flaccid bullae • initially containing clear yellow fluid • Nikolsky sign is absent • bullae quickly rupture, leaving a moist red surface, and then form thin, varnish-like light brown crusts
Staphylococcal Scalded Skin Syndrome • the most severe and systemic manifestation of infection with S. aureus strains producing an exfoliative exotoxin • The more general term toxic epidermal necrolysis is often used to encompass both SSSS and a morphologically similar syndrome of various causes (drug reactions, viral illnesses) • rarely develop in adults
Nikolsky sign can be demonstrated • Large, flaccid, clear bullae form, promptly rupture, and result in the separation of sheets of skin. • With appropriate fluid replacement and antimicrobial therapy, the skin lesions heal within 2 weeks, in contrast to drug-induced toxic epidermal necrolysis, in which recovery is more prolonged because the entire epidermis must be replaced and scarring is more frequent.
Treatment • Nafcillin or vancomycin • Systemic corticosteroids alone should not be used in the treatment of SSSS, although they may be indicated in therapy for drug-induced toxic epidermal necrolysis.
Toxic Shock Syndrome • acute febrile illness with a generalized scarlatiniform eruption associated with S. aureus infection. Other elements of the syndrome include (1) hypotension (shock), (2) functional abnormalities of three or more organ systems, and (3) desquamation
Folliculitis • pyoderma located within hair follicles • pruritic papules often topped by a central pustule • S. aureus is the usual cause • Diffuse folliculitis in 2 setting: 1- hot-tub folliculitis with Pseudomonas aeruginosafrom insufficently chlorinated swimming pools and whirlpools 2- swimmer`s itch( when skin exposed to water infested with schistosomiasiscercaria which penetrates ,die, elicit an allergic reaction)
Otitis externa is also a common manifestation • P. aeroginosa, enterobacteriace, candida • Malassezia furfur, a common skin saprophyte • Additional nonbacterial folliculitis( HSV, with Demodex mite infestation • Eosinophilic pustular folliculitis( in AIDS)
Local measures such as saline compresses topical antibacterial agents (e.g., mupirocin) or antifungal agents (e.g., clotrimazole
Folliculitis is a localized infection of hair follicles, which can extend into subcutaneous tissue, resulting in furuncles. These, in turn, may coalesce, leading to carbuncle formation
ULCER WITH OR WITHOUT ESCHAR • Cutaneous anthrax • Ulceroglandular tularemia • Mycobacterium ulcerans • Mycobacterium leprae • Mycobacterium tuberculosis
Anthrax • In the 20 years before 2001, naturally acquired anthrax infections, occurring in those working with raw imported wool, animal skins • sporadic cases still occur in transient workers in factories (e.g., ventilation repairmen) and in those who directly import wool for their own weaving
Most infections occur on the face, neck, or arms in an area with a minor abrasion. • Rarely, pulmonary infection occurs after inhalation of B. anthracis or • intestinal anthrax results from ingestion of the organism (e.g., after playing animal-skin drums). • A bioterrorism-associated anthrax outbreak occurred suddenly in the United States in 2001, when B. anthracis spores were mailed in letters to Washington, DC, New York City, and Florida. Twenty-two cases of anthrax ensued, 11 of the cutaneous form and 11 of the inhalation form.
Clinical Manifestations • incubation period of 1 to 8 days • painless, sometimes pruritic, papule develops on an exposed area. • The lesion enlarges, vesiculates (malignant pustule), and becomes surrounded by a wide zone of brawny, erythematous, gelatinous, nonpitting edema • As the lesion evolves, the initial vesicle enlarges and becomes hemorrhagic, necrotic, and covered by an eschar of variable dimensions
Malaise and low- • If untreated, bacteremic dissemination may occur, accompanied by high fever and hypotension. Meningitis may complicat bacteremic infection or primary pulmonary anthrax.
DDX 1-staphylococcal pustule or carbuncle with a necrotic escharmay be mistaken for early anthrax. However, the former is very painful and tender, and the causative agent can usually be demonstrated on a Gram-stained smear of material from the lesion 2-Ecthyma (usually lacking edema), ecthymagangrenosum (usually in neutropenic patients with P. aeruginosabacteremia) 3-brown recluse spider bite 4-orf (after exposure to sheep but without large eschar or gelatinous edema) 5- tick or mite bites (e.g., tularemia, rickettsial spotted fevers, scrub typhus).
TREATMENT • Incision and débridement should be avoided because they may increase the likelihood of bacteremia, but • skin punch biopsy after initiation of antimicrobial therapy may be necessary to establish the diagnosis by culture, immunohistochemical staining, or polymerase chain reaction (PCR) testing for B. anthraci
Almost all naturally occurring strains are susceptible to penicillin, and it has been the drug of choice for decades. • With the concern that bioterrorist attack strains might be weaponized to be resistant to penicillin (and other commonly used antimicrobial agents), the initial treatment of cutaneous anthrax with oral ciprofloxacin or doxycycline • has been recommended
Erysipelas • Now, 70% to 80% of erysipelas lesions involve the lower extremities and 5% to 20% are on the face. • Portals of entry may be skin ulcers, local trauma or abrasions, psoriatic or eczematous lesions,or fungal infections, but often the skin of the involved area is grossly intact. • by group A streptococci
painful lesion with a bright red, edematous, indurated(peau d’orange) appearance and an advancing, raised border that is sharply demarcated from the adjacent normal skin • Bullous erysipelas is a complication of severe disease that is observed in about 5% of cases
Differential Diagnosis • Early herpes zoster( pain preceding lesion) • contact dermatitis(absence of fever and the presence of pruritus) • familial Mediterranean fever • Diffuse inflammatory carcinoma of the breast • An erysipelas-like skin lesion was reported in several patients with hypogammaglobulinemia and Campylobacter jejuni bacteremia
Treatment • oral penicillin V (500 mg every 6 hours) or initial intramuscular procaine penicillin (600,000 units once or twice daily • Macrolides in allergic patients • Although typical erysipelas can be readily distinguished from cellulitis, which can be of staphylococcal or streptococcal origin, the differentiation occasionally may not be clearcut. Under such conditions, antistaphylococcal therapy (nafcillin, oxacillin, or a first-generation cephalosporin) should be considered
Cellulitis • acute spreading infection of the skin that extends deeper than erysipelas and involves the subcutaneous tissues • Group A streptococcus,other β-hemolytic streptococci, and S. aureus are the most common causative agents. • several days after the inciting trauma, local tenderness, pain,and erythema develop and rapidly intensify. Malaise, fever, and chills develop.
patchy involvement with skip areas • Regional lymphadenopath • bacteremia • Local abscesses • small patches of overlying skin may subsequently undergo necrosis • Staph aureous spreads from a central localized infection such as abscess,folliculitis or infected F.B. • in contrast strep. pyogen causes more rapidly spreading cellulitis with lymphangitis and fever
Recurrent strep. cellulitis of lower extremities in association with chronic venous stasis or saphenectomy or lymphedema • Recurrent staph. cellulitis among nasal carriers and among individuals who have eosinophilia and high serum level of IgE( job`s syn.) • H. influenza in periorbital cellulitis in association of sinusitis , OM
SPECIAL SETTINGS • Cat bite and to a lesser degree dog bite: pasteurella multocida, although in latter case staph. Intermedius and capnocytophaga canimorsus • Dog and human bite: anerobic such as fusobacteria, bacteriodes, aerobic and anerobic strep. and eikenella corrodens • Amoxiclavulonic , ampisulbactam,cefoxitin, tazocin are good choice for tx
Erysipelothrixrhusiopathiae is the causative agent of erysipeloid • in persons who handle saltwater fish, shellfish, poultry, meat • usually occurs in the summer • introduced through an abrasion on the hands • A painful violaceous area appears within 1 week after the injury. • distinct raised borders, the central portion • of the lesion clears. • Ulceration is not a feature. Occasionally, an adjacent • joint is involved; rarely, bacteremia and endocarditis may follow. • The causative organism is not usually observed in Gram-stained drainage from the lesion but may be isolated on culture of a biopsy specimen taken from the advancing margin of the lesion. • penicillin is the antibiotic of choice for the treatment of erysipeloid
NECROTIZING FASCIITIS Rapidly spreading destruction of skin, fascia, and muscles with associated systemic toxicity by: 1-Group A streptococcus 2-mixed aerob-anerobic bacteria 3- as part of gas gangrene by c. perfringens 4- MRSA
In type I necrotizing fasciitis, at least one anaerobic species (most commonly Bacteroides or Peptostreptococcus) is isolate in combination with one or more facultative anaerobic species, such as streptococci (other than group A) and members of the Enterobacteriaceae (e.g., E. coli, Enterobacter, Klebsiella, Proteus
In type II disease (also known as hemolytic streptococcal gangrene),group A streptococci are isolated alone or in combination with other species, most commonly S. aureus
CLINICAL MANIFESTATION • involving the subcutaneous soft tissues particularly the superficial (and often the deep) fascia • It is usually an acute process • most common on the extremities, particularly the legs • Extremity involvement is particularly common with type II necrotizing fasciitis; • abdominal wall, perianal and groin areas, and postoperative wounds are more common with type I (polymicrobial) infections.
The affected area is initially erythematous, swollen, hot, shiny, exquisitely tender, and painful • progresses rapidly over several days, with sequential skin color changes from red-purple to patches of blue-gray. • Within 3 to 5 days after onset, skin breakdown • with bullae (containing thick pink or purple fluid) and frank cutaneous gangrene (resembling a thermal burn) • By this time, the involved area is anesthetic secondary to thrombosis of small blood vessels and destruction of superficial nerves located in the necrotic, undermined subcutaneous tissue