Download
1 / 1
10 likes | 167 Views
Sensory Dysesthesia: Rare Presentation of Subependymoma. Mohankumar Kurukumbi 1 , Ganga Ramidi 2 , Swetha Samineni 2 , Alok Dabi 1 Annapurni Jayam-Trouth 1 . 1 Neurology, 2 Internal medicine, Howard University Hospital, Washington DC. Discussion

E N D
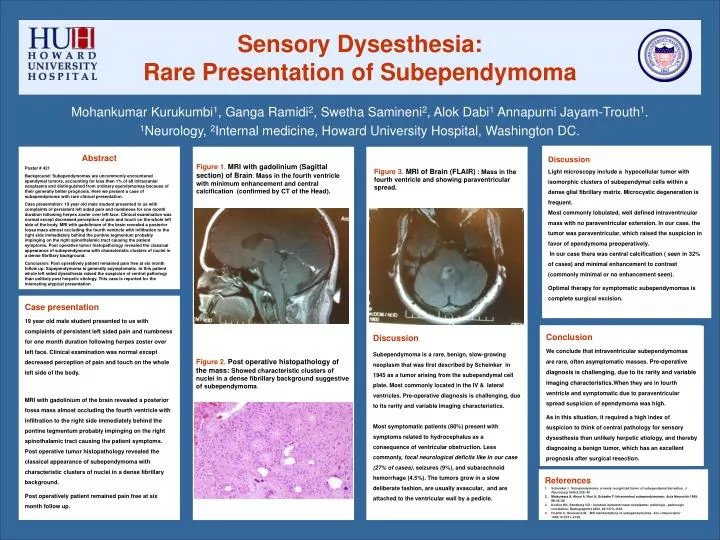
Sensory Dysesthesia: Rare Presentation of Subependymoma Mohankumar Kurukumbi1, Ganga Ramidi2, Swetha Samineni2, Alok Dabi1 Annapurni Jayam-Trouth1. 1Neurology, 2Internal medicine, Howard University Hospital, Washington DC. Discussion Light microscopy include a hypocellular tumor with isomorphic clusters of subependymal cells within a dense glial fibrillary matrix. Microcystic degeneration is frequent. Most commonly lobulated, well defined intraventricular mass with no paraventricular extension. In our case, the tumor was paraventricular, which raised the suspicion in favor of ependymoma preoperatively. In our case there was central calcification ( seen in 32% of cases) and minimal enhancement to contrast (commonly minimal or no enhancement seen). Optimal therapy for symptomatic subependymomas is complete surgical excision. Abstract Poster # 421 Background: Subependymomas are uncommonly encountered ependymal tumors, accounting for less than 1% of all intracranial neoplasms and distinguished from ordinary ependymomas because of their generally better prognosis. Here we present a case of subependymoma with rare clinical presentation. Case presentation: 19 year old male student presented to us with complaints of persistent left sided pain and numbness for one month duration following herpes zoster over left face. Clinical examination was normal except decreased perception of pain and touch on the whole leftside of the body. MRI with gadolinium of the brain revealed a posterior fossa mass almost occluding the fourth ventricle with infiltration to the right side immediately behind the pontine tegmentum probably impinging on the right spinothalamic tract causing the patient symptoms. Post operative tumor histopathology revealed the classical appearance of subependymoma with characteristic clusters of nuclei in a dense fibrillary background. Conclusion: Post operatively patient remained pain free at six month follow up. Supependymoma is generally asymptomatic. In this patient whole left sided dysesthesia raised the suspicion of central pathology than unlikely post herpetic etiology. This case is reported for theinteresting atypical presentation Figure 1. MRI with gadolinium (Sagittal section) of Brain: Mass in the fourth ventricle with minimum enhancement and central calcification (confirmed by CT of the Head). Figure 3. MRI of Brain (FLAIR) :Mass in the fourth ventricle and showing paraventricular spread. Case presentation 19 year old male student presented to us with complaints of persistent left sided pain and numbness for one month duration following herpes zoster over left face. Clinical examination was normal except decreased perception of pain and touch on the whole left side of the body. MRI with gadolinium of the brain revealed a posterior fossa mass almost occluding the fourth ventricle with infiltration to the right side immediately behind the pontine tegmentum probably impinging on the right spinothalamic tract causing the patient symptoms. Post operative tumor histopathology revealed the classical appearance of subependymoma with characteristic clusters of nuclei in a dense fibrillary background. Post operatively patient remained pain free at six month follow up. Conclusion We conclude that intraventricular subependymomas are rare, often asymptomatic masses. Pre-operative diagnosis is challenging, due to its rarity and variable imaging characteristics.When they are in fourth ventricle and symptomatic due to paraventricular spread suspicion of ependymoma was high. As in this situation, it required a high index of suspicion to think of central pathology for sensory dysesthesia than unlikely herpetic etiology, and thereby diagnosing a benign tumor, which has an excellent prognosis after surgical resection. Discussion Subependymoma is a rare, benign, slow-growing neoplasm that was first described by Scheinker in 1945 as a tumor arising from the subependymal cell plate. Most commonly located in the IV & lateral ventricles. Pre-operative diagnosis is challenging, due to its rarity and variable imaging characteristics. Most symptomatic patients (80%) present with symptoms related to hydrocephalus as a consequence of ventricular obstruction. Less commonly, focal neurological deficits like in our case (27% of cases), seizures (9%), and subarachnoid hemorrhage (4.5%). The tumors grow in a slow deliberate fashion, are usually avascular, and are attached to the ventricular wall by a pedicle. Figure 2. Post operative histopathology of the mass: Showed characteristic clusters of nuclei in a dense fibrillary background suggestive of subependymoma. • References • Scheinker I : Subependymoma: a newly recognized tumor of subependymal derivation. J Neurosurg 1945,2:232- 40 • Matsumara A, Ahyai A, Hori A, Schaake T: Intracerebral subependymomas: Acta Neurochir 1989, 96:15–25 • Koeller KK, Sandberg GD : Cerebral intraventricular neoplasms: radiologic– pathologic correlation. Radiographics 2002, 22:1473–1505 • Hoeffel C, Boukobza M, : MR manifestations of subependymomas. Am J Neuroradiol 1995,16:2121–2129.