Download
1 / 87
910 likes | 1.21k Views
Breast. Dr. Raid Jastania. Breast. Definitions: Lactiferous ducts, Duct, Lobule, Terminal duct lobular unit Common presentations of diseases Lump, mass, pain, skin changes Mammography: fibrous thickening and calcifications Triple test: Clinical, mammography, biopsy. Rare conditions.

E N D
Breast Dr. Raid Jastania
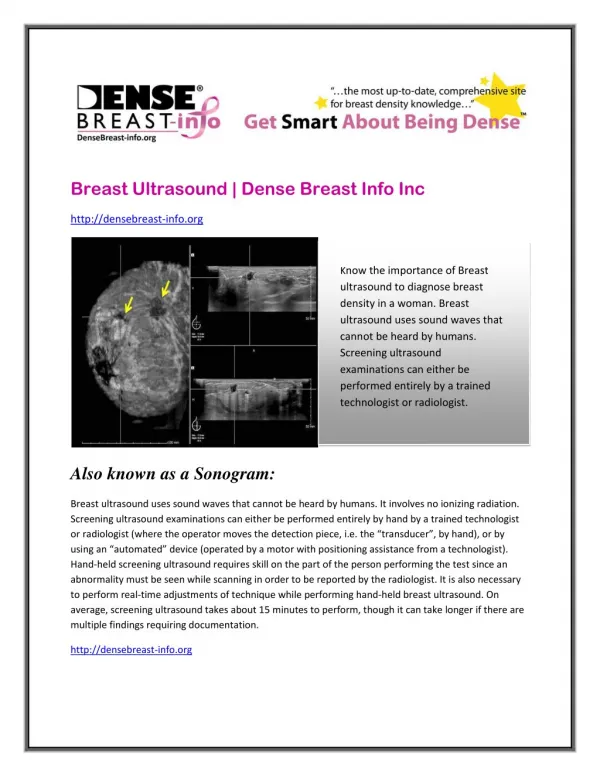
Breast • Definitions: Lactiferous ducts, Duct, Lobule, Terminal duct lobular unit • Common presentations of diseases • Lump, mass, pain, skin changes • Mammography: fibrous thickening and calcifications • Triple test: Clinical, mammography, biopsy
Rare conditions • Supernumerary nipples and breast • Congenital inversion of nipple • Galactocele
Fibrocystic Change • Present as mass or lump • Hormonal related, Estrogen • Types • Proliferative fibrocystic change • Non-proliferative fibrocystic change
Fibrocystic Change • Non-Proliferative fibrocystic change • Fibrosis • Cystic change • Apocrine metaplasia
Fibrocystic Change • Non-Proliferative fibrocystic change • Multifocal, bilateral • Nodularity, fibrosis • Cysts 1-5 com, Blue dome cysts, lined by benign epithelium, myoepithelial cells present, • Apocrine metaplasia • Calcification
Fibrocystic Change • Proliferative fibrocystic change • Epithelial hyperplasia • Sclerosing adenosis
Fibrocystic Change • Proliferative fibrocystic change • Epithelial hyperplasia • Types: Ductal, Lobular • Grades: Mild, moderate, severe (florid), atypcial • Sclerosing adenosis
Fibrocystic Change • Proliferative fibrocystic change • Epithelial hyperplasia • Sclerosing adenosis • Hard, rubbery • Fibrous stroma • Proliferation of small ducts (adenosis) with marked compression of the fibrous stroma (sclerosing)
Fibrocystic Change • Risk of Cancer: • Family history: double the risk
Carcinoma • Second to lung cancer as a cause of death • ¼ of women with the disease die • Lifetime risk is 1 in 8 women in US • Increasing incidence • 75% of patients are older than 50 y • 5% are younger than 40 y
Carcinoma • L > R (slightly) • 4% bilateral • Upper outer quadrant: 50% • Central zone: 20% • All other quadrants: 10% each
Carcinoma • Classification • Carcinoma In-situ • Ductal (DCIS) • Lobular (LCIS) • Invasive carcinoma • Ductal carcinoma (Scirrhous carcinoma) • Lobular carcinoma • Others: medullary, colloid, tubular…
Ductal Carcinoma In-Situ DCIS • Terminal duct lobular unit • Large malignant cells, monotonous, within ducts • Pattern • Solid • Cribriform • Papillary • Micropapillary • Comedo: central necrosis
Ductal Carcinoma In-Situ DCIS • Presentation • Mammography: calcifications • Can be palpable • Prognosis: 97% survival • 1/3 of cases progress to invasive cancer if untreated • Recurrence in 20-25%
Lobular Carcinom In-Situ LCIS • Terminal duct lobular unit • Uniform, monomorphic, bland, discohesive cells, some with vacuoles (signet-ring) • 1/3 will develop invasive cancer, the risk is to both sides of breast • LCIS is a marker of increased risk • Presentation: incidental, not palpable, no calcification
Invasive Ductal Carcinoma (NOS) or (NST) • 70-80% of invasive carcinoma • Associated with DCIS • Hard, palpable mass, irregular borders • Nipple retraction, Peau d’ orange • fixation to the chest wall
Invasive Ductal Carcinoma (NOS) or (NST) • Invasive adenocarcinoma • Irregular glands lined by malignant cells • Grading: tubular formation, nuclear grade, mitosis • 2/3 ER/PR + • 1/3 HER2/NEU over expression
Invasive Lobular carcinoma • 20% of invasive cancer cases • 2/3 are associated with LCIS • Most are palpable, but can be occult • More frequent multifocal, multicentric (10-20%)
Invasive Lobular carcinoma • Single cells, indian file, targetoid arrangement • Signet-ring cells, intracytoplasmic lumina • Matastasize to serosal surfaces and CNS, ovary • All ER/PR + • HER2/NEU over expression is rare
Medullary Carcinoma • Well circumscribed mass, pushing borders • Large anaplastic cells • Mixed with inflammatory cells • Cases of BRCA1 show medullary carcinom-like features • Lack ER/PR • HER2/NEU negative
Colloid carcinoma (mucinous) • Well circumscribed mass • Pools of mucus • Malignant cells floating in mucus • ER/PR + • HER2/NEU negative
Tubular carcinoma • Small <1cm • Irregular densities on mammography • Prognosis is excellent • ER/PR + • HER2/NEU negative
Inflammatory Carcinoma • Usually ductal carcinoma NOS • Clinical: enlarged swollen, erythematous breast • Cancer seen in lymphatic channels in skin • Poor prognosis