Download
1 / 49
510 likes | 828 Views
CHAPTER 16. Drugs, Addiction, and Reward Psychoactive Drugs. Psychoactive Drugs. Drug : a substance that on entering the body changes the body or its functioning. An agonist mimics or enhances the effect of a neurotransmitter.

E N D
CHAPTER 16 Drugs, Addiction, and Reward Psychoactive Drugs
Psychoactive Drugs • Drug : a substance that on entering the body changes the body or its functioning. • An agonist mimics or enhances the effect of a neurotransmitter. • An antagonist may occupy the receptors without activating them, simultaneously blocking the transmitter from binding to the receptors. • Psychoactive drugs are those that have psychological effects, such as anxiety relief or hallucinations.
Psychoactive Drugs: opiates • Opiates • derived form the opium poppy. • Can also be synthetically made • Act on opiate receptors or endorphin receptors • Several important effects: • analgesic (pain relieving) • hypnotic (sleep inducing) • produce a strong euphoria (sense of happiness of ecstasy). • Types of opiates: • Morphine: pain relief, surgical pain relief, cancer • Derivatives include codeine, vicodin, oxycotin, etc... • Heroin • synthesized from morphine • marketed as an over-the-counter analgesic until its dangers were recognized • now it is an illegal drug in the U.S.
Opiate drug action • Endorphins: • body produces its own natural opiates, which are neuromodulators • Released when in pain, motor exertion, stress • Endogenous opiates: • Endogenous = made by the body. • Opiate drugs are effective because they mimic endorphins • Because of CNS effects and cognitive effects, very high likelihood of abuse.
Psychoactive drugs: the depressants • Depressants: • drugs that reduce central nervous system activity. • Sedatives: calming drugs • Barbiturates including amobarbital (Amytal); pentobarbital (Nembutal); secobarbital (Seconal) and Phenobarbitol (Luminal) • Anxiolytic: anxiety-reducing drugs: • Benzodiazepines ("minor tranquilizers") including • Klonopin; diazepam (Valium); estazolam (Prosom); flunitrazepam (Rohypnol) ; lorazepam (Ativan) ; midazolam (Versed); nitrazepam (Mogadon) ; oxazepam (Serax) ; triazolam (Halcion); ;ttemazepam (Restoril; , Normison, Planum; Tenox, Temaze) ; chlordiazepoxide (Librium)
Psychoactive drugs: the depressants • Hypnotic drugs: induce sleep-like states: • Nonbenzodiazepines: • Zolpidem; Zaleplon; Zopiclone; Eszopiclone • Antihistamines: • Diphenhydramine; Doxylamine; Hydroxyzine; Promethazine • Others: • gamma-hydroxybutyric acid (Xyrem) • Glutethimide • Chloral hydrate • Ethchlorvynol • Levomepromazine • Chlormethiazole
Sedative effects on cns • Barbiturates • Suppress inhibitory centers • in small amounts: act selectively on higher cortical centers, especially those involved in inhibiting behavior • In low doses : • produce talkativeness • increased social interaction, • Higher doses: • sedatives and hypnotics. • Barbiturates do not reduce pain, but they do reduce the anxiety associated with pain. • Barbiturates produce their effects by decreasing glutamate activity and increasing GABA activity. • They operate at the barbiturate receptor on the GABAA complex.
Benzodiazepines- an alternative to barbiturates? • A few decades ago: • Barbiturates = drug of choice for treating anxiety • Also as most common drug for situations requiring sedation. • BUT: high liability • potential for addiction • High rate of accidental or intentional death. • Benzodiazepines: largelyreplaced barbiturates • produce anxiety reduction, • Also induce sedation and muscle relaxation. • operate at the benzodiazepine receptor on the GABAA complex. • At first, thought non-addictive • Today know that are highly addictive
Psychoactive drugs: Alcohol • Ethanol, or alcohol: • is a drug • fermented from fruits, grains, and other plant products. • Is a DEPRESSANT • It acts at many brain sites to produce euphoria, anxiety reduction, sedation, motor incoordination, and cognitive impairment • Why is it a depressant? • Depresses CNS • Inhibits areas of the brain that inhibit acting out, inappropriate behavior, etc..
How does alcohol affect the CNS? • Alcohol inhibits the release of glutamate (the most prevalent excitatory neurotransmitter). • glutamate reduction produces a sedating effect; • Chronic use results in a compensatory increase in glutamate receptors, • probably accounts for the seizures that sometimes occur during withdrawal. • Alcohol also increases the release of gamma-aminobutyric acid (GABA; • the most prevalent inhibitory neurotransmitter). • Alcohol specifically affects the A subtype of GABA receptor. • The combined effect at these two receptors is: • sedation, • anxiety reduction, • muscle relaxation, • inhibition of cognitive and motor skills.
Alcohol abuse effects • Cirrhosis of the liver, • Common side effect of chronic alcoholism • in its severest form is fatal. • Vitamin B1 deficiency • associated with chronic alcoholism • can produce brain damage and Korsakoff’s syndrome • Korsakoff’s syndrome • Neurological syndrome due to alcohol damage, B1 deficiency • involves severe memory loss along with sensory and motor impairment. • Alcohol withdrawal symptoms • involves tremors, anxiety, and mood and sleep disturbances; • Delirium tremors • more severe reactions • hallucinations, delusions, confusion, and in extreme cases, seizures • possible death.
Psychoactive stimulants • Stimulants: • activate the central nervous system to produce • arousal, • increased alertness, • elevated mood • Typically affect dopamine, norepinephrine and serotonin • Several drugs in this category • Cocaine • Amphetamine • Methamphetamine • Ritalin • Adderal, • Most ADHD medications • Ephedrine
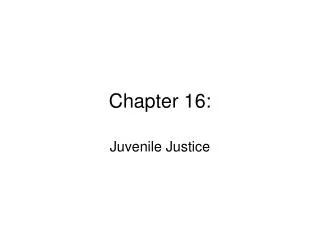
Psychoactive stimulants • Cocaine, • extracted from the South American coca plant, • produces • Euphoria • decreases appetite, • increases alertness • relieves fatigue. • Cocaine blocks the reuptake of dopamine and serotonin at synapses, • Potentiating effect of these neurotransmitters • Makes neurotransmitter remain longer in synapse. • Presumably, cocaine produces euphoria and excitement because dopamine removes the inhibition the cortex usually exerts on lower structures.
Cocaine user Normal
Psychoactive Drugs • Amphetamines • group of synthetic drugs • Again produce euphoria • increase confidence • concentration. • increase the release of norepinephrine and dopamine • Common examples: • Amphetamine (Adderal®); Dextroamphetamine (Dexedrine®, Dextrostat®) • Methamphetamine (Desoxyn®) • Highly related:Ritalin: • Ritalina, Rilatine, Attenta, Methylin, Penid, Rubifen); and the sustained release tablets Concerta, Metadate CD, Methylin ER, Ritalin LA, and Ritalin-SR. Focalin
Amphetamine Action • DA neurons release DA into the synapse: From there 1 of 3 things can happen: • DA can then attach to the post-synaptic membrane • DA can be degraded by enzymes • DA can be taken back up by the pre-synaptic membrane. • Amphetamine appears to affect all three mechanisms: • Promotes release of DA into the synapse • Inhibits the DA degredative enzyme, monoamine oxidase (MAO), • Blocks the uptake proteins in the pre-synaptic membrane • The result : Amphetamine effectively promotes a flood of DA into the brain reward center: • Nucleus Accumbens or Nac • This area is highly involved in both learning and reward.
Amphetamine Action • Amphetamine and related compounds elicit a variety of dose-dependent deleterious effects. • low doses of AMPH may improve attention and vigilance • improve vigilance • At high doses: over-stimulation of the motor and cognitive systems • behavioral stereotypy, repetitive thoughts and even hallucinations. • In rodents, a high AMPH dose elicits behavioral stereotypy: • continuous digging; Searching; Licking; Gnawing; Circling • In humans, high doses of AMPH may elicit: • psychotic state, • High rates of locomotion and repetitive behavior • high potential for self-injury or injury to others
Psychoactive Drugs: Nicotine • Nicotine: • primary psychoactive and addictive agent in tobacco • Also in chewing tobacco, nicotine gum, etc. • It stimulates nicotinic acetylcholine receptors. • In the periphery, • it activates muscles • may cause twitching. • In CNS: • produces increased alertness • Also faster response to stimulation.
Psychoactive Drugs: Caffeine • Caffeine: • active ingredient in coffee, many soda pops; teas; energy drinks, etc. • produces arousal, increased alertness, and decreased sleepiness. • Action: blocks receptors for the neuromodulator adenosine • This increases the release of dopamine and acetylcholine. • Because adenosine has sedative and depressive effects, blocking its receptors contributes to arousal • Acts like amphetamine in releasing DA.
PsychodelicDrugs • Psychedelic drugs: • compounds that cause perceptual distortions in the user. • May be referred to as hallucinogenic • Not really inducing hallucinations, but distortions in perception: • Light and color details are intensified, • objects may change shape, • sounds may evoke visual experiences, • light may produce auditory sensations.
Psychoactive Drugs • lysergic acid diethylamide (LSD) • best-known psychedelic • is structurally similar to serotonin • stimulates serotonin receptors • Appears to disrupt the brain stem’s ability to screen out irrelevant stimuli. • psilocybin and psilocin • Another serotonin-like psychedelics • both derived from the mushroom,Psilocybemexicana • Mescaline • the active ingredient in peyote (the crown or button on the top of the peyote cactus), • psychedelic properties result from stimulation of serotonin receptors.
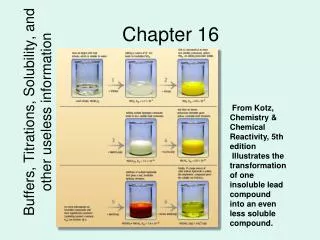
Psychoactive Drugs: Ecstasy • Ecstasy • street name for a drug developed as a weigh-loss compound • methlenedioxymethamphetamine (MDMA). • At low doses: • psychomotor stimulant • Increases energy, sociability, and sexual arousal. • At higher doses: • produces hallucinatory effects like LSD. • Also can overstimulate muscles resulting in “locked” or frozen muscles • MDMA stimulates • the release of dopamine which accounts for muscle and arousal effects • the release of serotonin, which probably accounts for the hallucinatory effects.
These brain sections have been stained with a chemical that makes neurons containing serotonin turn white. Photos in the top row are from a normal monkey; those below are from a monkey given MDMA a year earlier.
Psychoactive Drugs: PCP • Phencyclidine (PCP): • Developed as an anesthetic typically used by veterinarians • was abandoned for human use because it produces schizophrenia-like disorientation and hallucinations. • PCP increases activity in the dopamine pathways • This stimulates motivation system • Also, drug’s motivating properties apparently are partly due to its inhibition of a subtype of glutamate receptors.
marijuana • Marijuana • is the dried and crushed leaves and flowers of the Indian hemp plant, Cannabis sativa. • The major psychoactive ingredient is delta-9-tetrahydrocannabinol (THC) • . • THC actions: • THC binds with cannabinoid receptors, which ordinarily respond to endogenous cannabinoids. • Two known cannabinoids receptors: • anadamide • 2-arachidonyl glycerol, or 2-AG. • These receptors are found on axon terminals; • Unusual action: • cannabinoids are released by postsynaptic neurons • act as retrograde messengers, regulating the presynaptic neuron’s release of neurotransmitter.
Addiction • Reward refers to the positive effect an object or condition – such as a drug, food, sexual contact, and warmth – has on the user. • Drug researchers have traditionally identified the mesolimbicortical dopamine system as the location of the major drug reward system. • It takes its name from the fact that it begins in the midbrain (mesencephalon) and projects to the limbic system and prefrontal cortex. • The most important structures in the system are the nucleus accumbens, the medial forebrain bundle, and the ventral tegmental area.
Virtually all the abused drugs increase dopamine levels in the nucleus accumbens
Psychoactive Drugs • Addiction: • preoccupation with obtaining a drug • compulsive use of the drug in spite of adverse consequences • high tendency to relapse after quitting • Typically defined as an individual showing both withdrawal and tolerance. • Withdrawal: • negative reaction that occurs when drug use is stopped • Body’s compensatory reaction. • Tolerance: • individual becomes less responsive to the drug • requires increasing amounts of the drug to produce the same results.
Addiction • Societal definition: • obsession, compulsion, or excessive physical dependence or psychological dependence, • E.g., drug addiction, alcoholism, compulsive overeating, problem gambling, computer addiction, pornography, etc. • Scientific definitionof Addiction: Astate in which • the body relies on a substance for normal functioning and develops physical dependence • When the drug or substance on which someone is dependent is suddenly removed, it will cause withdrawal, • increased drug tolerance. • However, common usage spread to include psychological dependence, but brain doesn’t recognize this distinction
Addiction • Addiction and withdrawal take place in different parts of the brain and are independent of each other. • The ventral tegmental area is suggested to be involved in addiction, • Periventricular gray area produces classic signs of withdrawal. • Not mean that addicts never take drugs to avoid withdrawal symptoms, • Means that withdrawal is not necessary for addiction and avoidance of withdrawal is not an explanation of addiction.
Addiction involves Dopaminergic pathway • mesolimbicortical dopamine system • Major reward system • Many drugs (especially stimulants) mimic effects of normal reward. • begins in the midbrain (mesencephalon) and projects to the limbic system and prefrontal cortex. • The most important structures in the system: • nucleus accumbens • medial forebrain bundle • ventral tegmental area.
Reward and the Dopaminergic pathway • Schultz (2005) and others show: • Dopamine is not released as a reward • Dopamine is a motivating neurotransmitter- produces increases in locomotion, action behavior that is oriented towards reward • Thus: when dopamine released, body moves towards or continues doing whatever it was doing to keep getting that “Reward” • General DA reward system serves as feedback system that identifies • need to continue or shift behavior depending on reward situation • Helps select the appropriate response for the situation
Changing behavior with DA agonists • Virtually all the abused drugs increase dopamine levels in the nucleus accumbens. • Electrical stimulation of the brain (ESB), • Stimulate Nucleus accumbens • Animals press a level or engage in high rates of locomotion immediately after receiving stimulation • Why? DA release elicits “search” behavior • A reinforcer is any object or event that increases the probability of the response that precedes it • Thus, must keep doing the behavior that got you the reinforcer • DA maintains ongoing responses or kicks you into movement behaviors that increase likelihood of reward.
Changing behavior with DA agonists • Think of symptoms of stimulant abuse/addiction: • Lots of motor movement • Lots of perseverative motor behavior: • Nose wiping • Tics • Perseveration • Paranoia is highly similar to schizophrenia • Why? Too much dopamine is overstimulating circuits, cognitive areas of brain are hyperstimulated. • What got you these feelings- the drug • What do to keep these feelings- get more drug • And, because you have replaced normal DA levels, now you will engage in seeking behaviors to maintain those levels!
Diminished dopamine? • Chronic drug users show diminished DA release from DA receptors • May be individual, and not the addiction • Lower levels of D2 autoreceptors • Note that those with high number of D2 autoreceptors find DA drugs unpleasurable; those with fewer report more pleasure • D2 autoreceptors help regulate general DA tone in synapse, regulate reuptake and production of DA • Thus, may be that DA-drug addicts have reward deficiency syndrome: insufficient receptors to respond to DA, need more DA to get same effect
Step down reflex • Addiction = learning • Learning produces changes in the brain • Addiction produces same changes • Drug = release of DA: • US(drug) UR(drug effects) • Stimulus (CS) predicts drug that releases DA: • CS(cue US(drug) UR(drug effects) • Anticipate DA release BUT Body prefers homeostasis: no sudden changes, maintain level • CS(cue US(drug) UR(drug effects) \ CR(decrease DA release in anticipation of drug DA release) Thus: body REDUCES dopamine in ANTICIPATION of increase in DA
Compensation: tolerance and withdrawal • Body REDUCES dopamine in ANTICIPATION of increase in DA • No longer get same effect for drug • Must take more • This is called tolerance • If stop taking the drug, no step-down reflex or compensation • Now, reduction in DA • Now have too little DA: shaky, motor tremors, etc. • This is called withdrawal: Setting cues are critically important
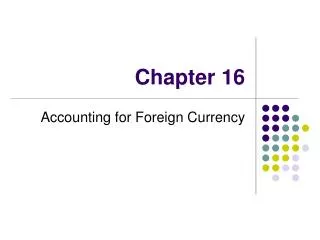
PET scans are shown at two depths in the brain. Notice the increased activity during presentation of cocaine-related stimuli. Frontal areas (DL, MO) and temporal areas (TL, PH) are involved in learning and emotion.
Evidence for Addiction? • Nora Volkow and her colleagues, among others • Transition from controlled drug use to compulsive drug intake involves pathological changes in communication between prefrontal cortex and the nucleus accumbens. • addict returns to drug taking when stress or drug-related stimuli trigger increases in dopamine release in the prefrontal cortex and glutamate release in the nucleus accumbens. • Prefrontal release produces a compulsive focus on drugs at the expense of other reinforcers • Glutamate release cranks up the drive to engage in drug seeking.
Treating Addiction • Agonist treatments replace an addicting drug with another drug that has a similar effect. • Opiate addiction is often treated with a synthetic opiate called methadone. • Antagonist treatments involve drugs that block the effects of the addicting drugs. • Drugs that block opiate receptors are used to treat opiate addictions and alcoholism because they reduce the pleasurable effects of the drug. • Antabuse for alcohol • Another experimental strategy is to interfere with the dopamine reward system. • Baclofen reduces dopamine activity in the ventral tegmental area by activating GABAB receptors on dopaminergic neurons.
The Role of Genes in Addiction • If genetics plays such an important role in addiction, just what is inherited? • Most research on the genetics of addiction implicates various neurotransmitter systems. • Appears to be a syndrome or related group of dysfunction • Addicts correlated with individuals who have family members with • Schizophrenia, bipolar disorder, depression • ADHD and related disorders • Autism and autism-spectrum disorders.
The Role of Genes in Addiction • Dopamine is one of the factors differentiating addictive from normal behavior. • There are several alleles, or alternate forms, or the gene responsible for the development of the D2 subtype of dopamine receptor. • Various alleles are associated with alcoholism, cocaine dependence, stimulant abuse, and multiple addictions. • Serotonin is involved in drug abuse in general • Also in mood, • sexual behavior, • aggression, • the regulation of bodily rhythms and food and water intake. • Bottom line: May have a predisposition • Stress bring out or turns on different coping mechanism • Best way to avoid: reduce stress; avoid situations with drug availability
A Societal comment on drug usage from the onion! And now for something absolutely silly! http://www.theonion.com/content/video/fda_approves_depressant_drug_for