Download
1 / 16
170 likes | 546 Views
MC congenital anomalies = abnormal variants of the gallbladder MC= folded fundus ( Phrygian cap ) Others= congenitally absent, bilobed or aberrantly located gall bladder. Most common congenital anomaly. Cholelithiasis ( Gall Stones) 10 to 20% of adults in developed countries

E N D
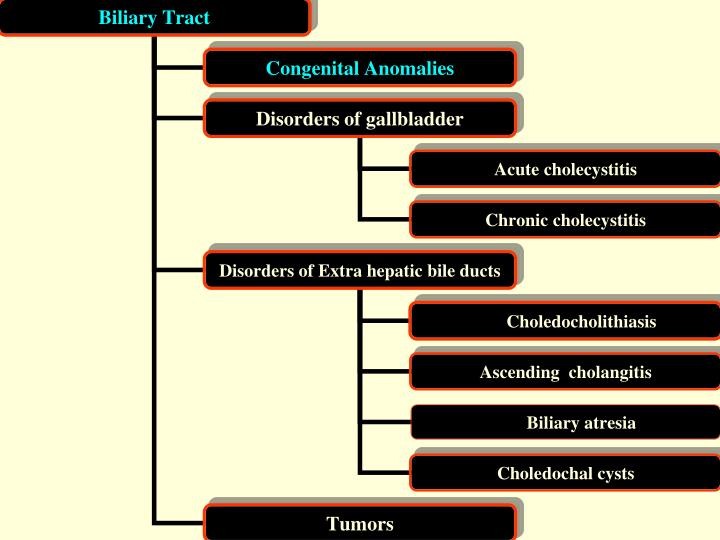
MC congenital anomalies= abnormal variants of the gallbladder • MC= folded fundus (Phrygian cap) • Others= congenitally absent, bilobed or aberrantly located gall bladder Most common congenital anomaly
Cholelithiasis (Gall Stones) • 10 to 20% of adults in developed countries • Two kinds of stones • 1. Cholesterol Stones= crystalline cholesterol monohydrate, • Risk factors • Native American • adult in industrialized country • increased age (>40 yrs, Forty) • Females 2:1 • estrogenic influences (Fertile) • Clofibrate • Obesity (Fatty) or rapid weight loss • Gallbladder stasis, • in spinal cord injury • pregnancy • Hypercholesterolemic syndromes
1. Cholesterol Stones contd… • Four conditions -necessary for cholesterol stone formation • supersaturated bile with cholesterol • gallbladder hypomotility promotes crystal nucleation • microprecipitates of calcium salts (inorganic or bilirubin salts) • Mucus hypersecretion in the gallbladder • Morphology= Pale yellow and hard, ovoid, usually single, Often radiolucent • Cholesterol stones arise exclusively in the gall bladder • 2. Pigmented Stones=bilirubin calcium salts • Risk factors • Asian, Rural • Chronic hemolytic syndromes • Biliary tract infection (E. coli, Ascaris lumbricoides, liver fluke -Opisthorchis) • Ileal disease (resection or bypass) • Cystic fibrosis with pancreatic insufficiency • Mechanisms=↑ Unconjugated bilirubin in the biliary tree and precipitation of calcium bilirubin salts • Morphology = more often radiopaque, black color • Clinical( both types)= 70 to 80% of gallstone patients -asymptomatic
Clinical( both types) • Symptoms • spasmodic, colicky pain, owing to obstruction of bile ducts by passing stones, • gallbladder obstruction per se generates right upper abdominal pain, • Complications= cholecystitis,Empyema, perforation, fistulas, cholangitis, Obstructive cholestasis or pancreatitis and , gallstone ileus, Mucocele • other sites of Mucocele?
Acute Cholecystitis =acute Inflammation of the gallbladder • Cause = MCC gallstone obstruction of the neck or the cystic duct(90% ) • Rarely without gallstone obstruction (10%)- severely ill patients (ex. in the postoperative state, severe trauma, severe burns, multisystem organ failure, sepsis, prolonged hyperalimentation or postpartum state) • Symptoms of CBD obstruction = acute right upper quadrant or Epigastric pain, mild fever, anorexia, tachycardia, diaphoresis, nausea and vomiting, jaundice • Patho –Mechanisms = bile acids (in cholelithiasis pts.) chemical irritation of gallbladder inflammatory mediators (lysolecithin, prostaglandins) • in the severely ill patient= direct result ofischemia • Gross=enlarged, tense gallbladder , fibrin on serosal covering • Course = mild and intermittent or may be a surgical emergency, • self-limited and mortality is less than 1%, or severely ill patient with mortality is higher, • complications • cholangitis and sepsis • gallbladder perforation or rupture • enteric fistula formation
Chronic Cholecystitis • Causes= MCC from repeated bouts of symptomatic acute cholecystitis or • Morphology =fibrosed, contracted gallbladder, GB wall - thickened and gray-white • Microscopy =mucosa is preserved • Cholesterolosis =cholesterol-laden macrophages in the lamina propria • Gallstones • Rokitansky -Aschoff sinuses =Mucosal out pouching • porcelain gallbladder = rarely - dystrophic calcification • xanthogranulomatous cholecystitis =Fibrosed, nodular & histiocytic inflammation of gallbladder • Clinically = steady or colicky Recurrent attacks of Epigastric or right upper quadrant pain • Complications= same as acute
Choledocholithiasis = Stones within the biliary tree • in about 10% of patients with cholelithiasis • Western nations - almost all stones are derived from the gallbladder (cholesterol stones) • Asia- stones are usually primary and pigmented • Symptoms arise from • obstruction • pancreatitis • cholangitis • hepatic abscess • secondary biliary cirrhosis • acute calculous cholecystitis • Ascending Cholangitis = Bacterial infection of the bile ducts, • Common in the setting of Choledocholithiasis, • Ascending bacteria (E. coli, Klebsiella and other enterobacteria) enter the biliary tract through the sphincter of Oddi
Extrahepatic Biliary Atresia = Complete obstruction of bile flow • unknown cause • Mechanism = destruction or absence of all or part of the extrahepatic bile ducts • Normal at birth , later progressive inflammatory destruction • Liver changes (same as cholestasis) • marked bile duct proliferation • portal tract edema and fibrosis • Cirrhosis within 3 to 6 months • Clinical features= neonatal cholestasis with normal birth weight & postnatal weight gain • Treatment= liver transplantation is curative • if untreated, death occurs within 2 years of birth • Choledochal Cysts • congenital dilations of the CBD in Children < ten yr. age • Clinically = Jaundice, recurrent abdominal pain • Complications • Predispose to = stone formation, stenosis and stricture, pancreatitis, • in the adult life = Obstructive biliary complications and bile duct carcinoma
Carcinoma of Gall Bladder (GB)= F>M, in their 60's • Gallstones coexist in patients in Western nations • critical risk factor=Chronic inflammation of GB • MC- adenocarcinomas • unresectable when discovered • prognosis really is BAD • Extahepatic Bile Duct Carcinoma = uncommon malignancies of the extrahepatic biliary tree down to the ampulla of Vater • Risk factors • choledochal cysts & Calori disease • ulcerative colitis, • Biliary infection with C. sinensis • MC- adenocarcinomas, • Klatskin's tumors • tumors arising at the confluence of the right and left hepatic bile ducts • notable for slow growth, • sclerosing behavior and • infrequency of distant metastasis • Good Prognosis