Download
1 / 74
750 likes | 936 Views
The Emerging Role of Adipose Tissue. Gareth Denyer University of Sydney, Australia. Obesity in Australia. Epidemiology of obesity World perspective. 50% European adults 35-65 years old are overweight or obese More men overweight, more women obese

E N D
The Emerging Role of Adipose Tissue Gareth Denyer University of Sydney, Australia
Epidemiology of obesity World perspective • 50% European adults 35-65 years old are overweight or obese • More men overweight, more women obese • In Western countries, inversely associated with socio-economic status UK Foresight study Female Class V 30 For Aus stats: www.asso.org.au navigate to fast facts Male Class V 20 Male Class I Female Class I 10 ‘93 ‘06
The Propaganda • We are second only to USA • 52% of Australian women & 67% Australian men are overweight or obese. • 2.5 times higher than in 1980. • Childhood obesity in Australia one of the highest amongst developed nations. • 25% overweight or obese. • Health crisis costing $1.5 billion a year in direct health costs • “Fattest people are getting fatter faster” • “2050 90% adults and 40% children overweight” From www.asso.org.au
Alternative View • The recent rise is not as rapid as before • Greatest rise was 15 years ago • Speakman Int J Obes (2008) 32 1611-7 • We are all just reaching our ‘set point’ • Previously exercise and low-calorie foods kept us below the set point • In the past, only the very rich were fat! • In developing nations, higher classes fatter
Health Risks of Obesity in Adults Nurses’ Health Study (women 30 to 55 yr) Health Professionals Follow-up Study (men 45-60 yr) Women Men Relative Risk Body Mass Index
Morbidity and Mortality • Increased mortality and morbidity • >20% of deaths from coronary heart disease • >70% of cases of Type 2 diabetes • Chronic Disease • Dyslipidemia • Arthritis • PCOS - polycistic ovarian disease • Sleep apnoea • Hypertension • NAFLD/NASH • non-alcoholic fatty liver disease, steatohepatitis
Circulating CVD factors characteristic of obesity • High cholesterol • Low HDL, high LDL • Other dyslipidemia • Triglyceride concentration • Small, dense LDLs • Elevated apoB • Prothrombotic factors • High Systolic Blood Pressure • Proinflammatory markers
In NSW – 25% of boys and 23% of girls are overweight or obese (2004) Health concerns associated with childhood obesity are similar to adults Ebbeling. Pawlak, Ludwig: Lancet, 2002
Social and Cultural Impact • Obviously very difficult to do these studies • All MUST be adjusted for socioeconomic status • But several done in Australia • Employment • wage ‘penalty’ of up to 12% • Health Care • reluctance to seek health care services • reluctance for doctors to discuss weight with patients • ‘too difficult’, ‘non-compliant’ • Education • lower university and tertiary education attendance • Relationships • interesting studies with assessment of ‘blind’ interactions vs photo-prompted
Social Networks children – peer harassment and rejection
Problem with BMI? • Classification by Body Mass Index (BMI) • obese > 30 kg/m2 • overweight > 25 kg/m2 • May not apply to all ages and shapes • Waist & waist:hip ratio • Alert – • Men > 94 cm (37 in), WHR > 0.95 • Women > 80 cm (32 in), WHR > 0.8 • Action – • Men > 102 cm (40 in) • Women > 88 cm (35 in)
Men have more visceral fat 250 ♂ 150 VAT (area, cm2) ♀ 50 10 20 30 40 50 60 % fat
Racial Differences too… Lancet, 2003 % fat and VISCERAL FAT also higher per BMI in Caucasian men, African American women and both genders of Asian’s and Indians
Lower Body Normal Obesity and Coronary Artery Disease Upper Body 100 80 60 12 y CAD Risk/1000 40 20 0 BMI Tertiles Non-obese Overweight Obese Honolulu Heart Study: 7692 men, 12 yr follow-up Donahue RP, Lancet 1987;1(8537):821-4
Visceral Fat and Glucose Intolerance Glucose Insulin mM nM 12 12 Upper Body Obesity 9 9 6 6 Lower Body Obesity Controls 3 3 0 0 0 1 2 3 0 1 2 3 Time (h) Time (h) Despres et al (1995) Int J Obes 19; S76
Visceral/Subcutaneous • Fat distribution • gluteo-femoral fat – no problems • abdominal viscera - diabetes & coronary artery disease. • independent of age, overall obesity or the amount of subcutaneous fat. • New definition of obesity? • based on the anatomical location of fat rather than on its volume, • Metabolic Obesity • visceral fat accumulation in either lean or obese individuals
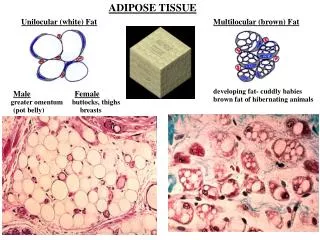
The Old (!!) view Adipose as Connective Tissue • “The individual cells fill up with fat and the cytoplasm and the nucleus are pressed to the edge of each cell membrane.” • “Adipose can be found under the skin, on the heart, and around the kidneys. It serves to protect, insulate, and store fat.”
Metabolic Warehouse? Uptake of Fat after a meal Synthesis of Fat in response to insulin Releasing fatty acids into the bloodstream during starvation and exercise Very dynamic – huge fluxes after meals & during starvation Adipocyte size is very flexible
Obesity - Metabolic Inflexibility Activity of Visceral fat in fasted subjects Meal (100 g carbohydrate) 15 normal FA release (nmol/ml/min) obese • Obese vs. normal • Less suppression after meal • Continual release even when fed • Less release during fasting 0 0 300 Time after meal (min)
NEFA Control • Fatty acid buffering is reduced in obesity • Overspills into the other tissues • inappropriate accumulation of fat in muscles and liver • leading to insulin resistance and steatosis • Visceral fat especially good at releasing NEFA • Into portal circulation so to liver first • especial effect on glucose and VLDL output
New viewLargest Endocrine Organ!! LIPOSTAT ADIPOSTAT Leptin Hypothalamus Leptin Receptors Energy Intake Metabolic Rate Adipocytes Fat Storage
Early Enthusiasm for Leptin Before After • People without leptin are hyperphagic • ..and they respond to leptin injections 100 Leptin Body Weight (kg) 50 0 0 3 6 9 Age (years) So could leptin injections be the ‘cure’ for obesity?
Leptin and Obesity 100 • Obese people higher blood [leptin] • More and bigger WAT cells • Leptin higher in women • Sex hormone interactions • Extra leptin is ineffective • leptin-resistant… why? • Small changes in leptin may not be meaningful • Rather than a excess of leptin telling us to stop eating, a lack of leptin may tells us to start eating Serum Leptin (ng/ml) 50 0 0 20 40 60 Body fat (%)
Adipokines – molecules secreted by adipose tissue • Leptin receptors are like cytokine receptors • Adipocytokines… Adipokines • Many more discovered! • Affecting more than just appetite and metabolic rate • Over 50 known protein and signal molecules
LIPID METABOLISM APPETITE BLOOD PRESSURE Cholesterol ester transfer protein leptin angiotensin IMMUNITY ANGIOGENESIS complement proteins (adipsin) VEGF INSULIN SENSITIVITY adiponectin resistin visfatin INFLAMMATORY CYTOKINES TNF-α Interleukin-6 C-reactive protein HEMOSTASIS PAI-I (plasminogen activator inhibitor-I) CELL ADHESION intercellular adhesion molecule -1 Lots of Adipokines
WAT is not all Adipocytes • Other cells comprise adipose tissue • stromal-vascular cells • pre-adipocytes (stem cells) • macrophages • Macrophages also secrete a range of cytokines • So the adipokines coming from WAT may not always be adipocyte-derived • Resistin best example • rodents in adipocytes, macrophages in humans
Obesity as Inflammation • Big fat cells and big fat pads produce large amounts of adipokines • except adiponectin • adiponectin produced by small fat cells • As fat stores get bigger • increased mix of inflammatory cytokines • increased blood coagulation potential • increased blood pressure • WAT is potentially the BIGGEST endocrine organ! • Affecting many tissues and homeostatic processes
Adipokines of Interest • Inflammatory cytokines • the link between adiposity and heart disease? • Interleukin-6 – high in obese. More from visceral. • Plasminogen activator inhibitor 1 (PAI-1) – high in obese • C-reactive protein - liver and also in adipose tissue • Adipokines that affect insulin sensitivity • the link between adiposity and Type II diabetes? • TNF-α – insulin resistance in muscle (IRS interference) • visfatin – produced by visceral fat • adiponectin – produced by small adipocytes • Inflammatory and resistance markers especially raised in VISCERAL ‘obesity’ • but cause or effect?
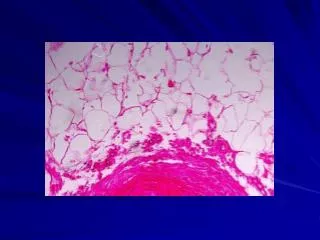
Macrophages 60 • 10% of cells in WAT • Much higher in obese fat pads • More “activated” in obese • Even fuse to form giant • multinuclear cells • Source? • Stem cells in WAT can become macrophages • But likely to be trapped by increased local expression of ICAM-1 • Macrophages really similar to adipocytes • Both can carry fat (remember foam cells) • May be there to mop up fat from large, burst cells 40 % macrophages 20 0 0 5,000 10,000 Average adipocyte area (µm2)
Dying Fat Cells Macrophages (green) Cluster around fat cell
Not all adipokines are proteins… • Cell 134, 933–944, September 19, 2008 Systemic lipid profiling also led to identification of C16:1n7-palmitoleate as an adipose tissue-derived lipid hormone that strongly stimulates muscle insulin action and suppresses hepatosteatosis.
WAT affects other tissues • WAT is the most insulin sensitive tissue • Although total responsiveness is not great • Metabolically relatively inactive • Glucose disposal slow in comparison to muscle • Low contribution to glucose disposal on a whole body basis • BUT fatty acid and adipokine release affects insulin action in other tissues • Even in normal weight people, WAT can be 25% of body weight • Can range from 3% (male elite athlete) to 70% (very obese)
Examples • Anti-diabetic thiazolidinedione drugs • increase insulin sensitivity in WAT • Change the adipokine profile • Increase production of new fat cells which produce adiponectin • Knockout of GLUT-4 in WAT • Widespread insulin resistance in muscle and liver • Even though WAT size unaffected
Effects of WAT loss • Lipodystrophy • Lack of adipose tissue • Accompanied by • Insulin resistance • Type II diabetes • Dyslipidemia (high triglycerides, low HDL) • Hepatic and muscle fat accumulation • Hepatic steatosis and cirrhosis • Some sexual abnormalities • Lack of ovulation, infertility • Excess of male hormones hirsuitism
Lipodystrophies • Inherited • Defects in genes that control adipocyte development • Acquired • HIV patients receiving protease inhibitors • >100,000 protease-induced lipodystrophies in USA • Impairment of adipocyte differentiation • But only in some depots • Loss of subcutaneous fat in face, arms, legs • Others depots compensate • Exaggerated shapes (eg, thin, drawn face, very wide hips) • Sleep apnoea after HIV treatment • International Journal of STD & AIDS 2006; 17: 614–620
Transplantation • Removal of fat from one site • Compensatory increase in size of other depots • Dynamic • In hibernating animals or animals in which fat is laid down ‘seasonally’ the “correct” level of fat is re-made • Grafting experiments • Pads grafted are not ‘noticed’ by the animal • No compensatory changes – not ‘lipostatically’ active • UNLESS… • Donor pads are grafted touching another pad… • Implies paracrine interactions between the pads
Whole Body Effects • Transplant WAT into lipoatrophic animals • Restores glucose tolerance • But the transplanted fat has to be good “quality” • Small, active adipocytes good • Triglyceride laden, old adipocytes do not help • Transplantation of young, insulin sensitive adipocytes into insulin resistant animals • Restores glucose tolerance • Subcutaneous/visceral transplants • Show depots are intrinsically distinct • More subcutaneous improves insulin sensitivity
Does fat cell number change? • Nature 2008 June 5; 453(7196) p783-7 The number of fat cells stays constant in adulthood in lean and obese individuals, even after marked weight loss. The number of adipocytes is set during childhood and adolescence. Approximately 10% of fat cells are renewed annually at all adult ages and levels of BMI.
Spalding, 2008 Nature obese lean
Hyperplasia and Hypertrophy even with 6 months calorie restriction, no apoptosis weight loss cell number constant HYPERTROPHY HYPERPLASIA?? regain weight gain adipocytes larger potential for fat deposition?