Download
1 / 17
180 likes | 332 Views
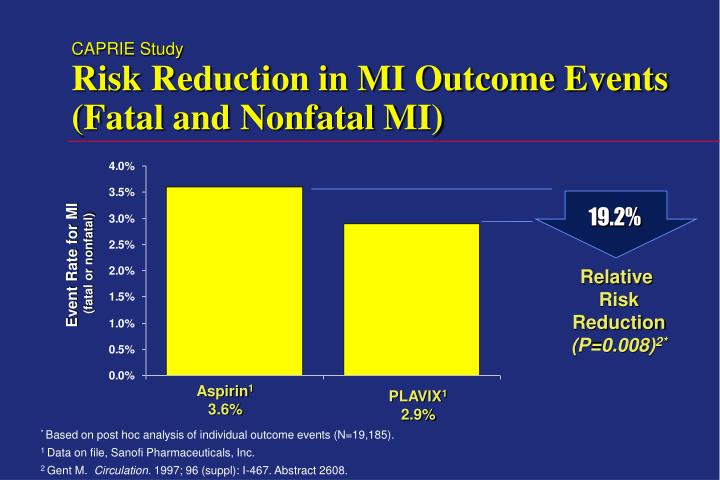
CAPRIE Study Risk Reduction in MI Outcome Events (Fatal and Nonfatal MI). 19.2%. Event Rate for MI (fatal or nonfatal). Relative Risk Reduction (P=0.008) 2*. Aspirin 1 3.6%. PLAVIX 1 2.9%. * Based on post hoc analysis of individual outcome events (N=19,185).

E N D
CAPRIE StudyRisk Reduction in MI Outcome Events (Fatal and Nonfatal MI) 19.2% Event Rate for MI (fatal or nonfatal) Relative Risk Reduction (P=0.008)2* Aspirin1 3.6% PLAVIX1 2.9% * Based on post hoc analysis of individual outcome events (N=19,185). 1 Data on file, Sanofi Pharmaceuticals, Inc. 2 Gent M. Circulation. 1997; 96 (suppl): I-467. Abstract 2608.
19.2% RelativeRiskReduction CAPRIE StudyRisk Reduction in MI Outcome Events (Fatal and Nonfatal MI) Aspirin 5 Clopidogrel Aspirin1 3.6% 4 (P = 0.008)2* Event Rate for MI (%) (fatal or nonfatal) 3 2.9% Clopidogrel1 2 1 0 36 3 6 9 12 15 18 21 24 27 30 33 Months of Follow-Up * Based on post hoc analysis of individual outcome events (N=19,185). 1 Data on file, Sanofi Pharmaceuticals, Inc. 2 Gent M. Circulation. 1997;96(suppl):I-467. Abstract 2608.
CAPRIE StudyAdditional Manifestations of Atherosclerosis Prior to Study Entry (n=5833) Prevalence (%) in the CAPRIE population (n=3205) (n=1689) (n=1534) (n=851) * Does not include the qualifying event/condition. CAPRIE Steering Committee. Lancet. 1996;348:1329-1339. Data on file, Sanofi Pharmaceuticals, Inc.
CAPRIE StudyAdditional Cardiovascular Risk Factors At Study Entry (n=9885) (n=7904) Prevalence (%) in the CAPRIE population (n=5668) (n=3881) CAPRIE Steering Committee. Lancet. 1996;348:1329-1339. Data on file, Sanofi Pharmaceuticals, Inc.
Current Labeling for Oral Antiplatelet Agents Plavix Ticlid Aspirin Yes Yes No Recent Ischemic Stroke Yes No Yes Recent Myocardial Infarction Yes No No Established PAD Plavix Package Insert. Ticlid Package Insert. Aspirin Professional Labeling.
CAPRIE StudyMI Paradox: Subgroups vs. Outcomes Relative Risk Reduction* by Qualifying Subgroup1 Relative Risk Reduction of Individual Outcomes in Total Population IS MI PAD Total Aspirin better Clopidogrel better 7.3% 5.2% 2 IS (fatal or non-fatal) MI (fatal or non-fatal) Vascular death Total Aspirin better Clopidogrel better -3.7% 19.2% 3‡ 23.8% 7.6%1 8.7%1† 8.7%1† -40 -20 -10 0 10 20 30 40 -40 -20 -10 0 10 20 30 40 *Cluster of IS, MI, or vascular death † p=0.043 ‡ p=0.008 1 CAPRIE Steering Committee. Lancet.1996; 348:1329-1339 2 Easton JD. Neurology. 1998 July; P03.081 Abstract. 3 Gent M. Circulation. 1997; 96(8 supple): I-467 Abstract.
19.2% RelativeRiskReduction CAPRIE StudyRisk Reduction in MI Outcome Events (Fatal and Nonfatal MI) Aspirin 5 Clopidogrel Aspirin1 3.6% 4 (P = 0.008)2* Event Rate for MI (%) (fatal or nonfatal) 3 2.9% Clopidogrel1 2 1 0 36 3 6 9 12 15 18 21 24 27 30 33 Months of Follow-Up * Based on post hoc analysis of individual outcome events (N=19,185). 1 Data on file, Sanofi Pharmaceuticals, Inc. 2 Gent M. Circulation. 1997;96(suppl):I-467. Abstract 2608.
CAPRIE StudyNet Benefit of Clopidogrel: Prevention of Atherosclerotic Events and Major Bleeding Complications • Primary Hemorrhagic Intracranial Cluster* Death Hemorrhage Total Events RRR‡‡ • Clopidogrel 939 4 34 977 • Aspirin 1021 2 47 1070 Safety Endpoints Efficacy Endpoint Net Benefit 9.5% * First outcome event of ischemic stroke, myocardial infarction, and vascular death ‡‡ Relative Risk Reduction (p=0.025) Easton JD. American Academy of Neurology. 1998 April; 50(4): Abstract.
CAPRA AnalysisCaprie Actual Practice Rates Assessment • ObjectiveTo estimate the event rates expected in actual practice vs. CAPRIE population. • Patient Population 9,072 patients with MI, ischemic stroke, or PAD in Saskatchewan, Canada. • Results First Hospitalized Event RateASA ClopidogrelMI 6.4% 1.9% Stroke 5.8% 2.6% All cause death 9.7% 3.1% • Conclusion Ischemic events occurred between 2 - 3.4 times more often in actual practice. Translates to 15 additional events prevented by clopidogrel over aspirin per 1,000 patients treated per year. Caro J. Euro Heart J. 1998;19: P1263 Abstract.
CAPRIE StudyConsistency of Clopidogrel Benefit Across Atherosclerotic-Related Events • RRR (95% CI)Single endpoints:IS 5.2 (-7.9 - 16.7) MI 19.2 (5.3 - 31.0) Vascular death 7.6 (-6.9 - 20.1)Combined endpoints of vascular events: IS, MI 10.9 (1.5 - 19.5) TIA, hospitalization due to angina 7.5 (-1.2 - 15.5) IS, MI, TIA, hospitalization due to angina 7.9 (1.5 - 13.8) • Combined endpoints of major vascular events:Any stroke*, MI, vascular/hemorrhagic 9.5 (1.3 - 17.0) death (net benefit cluster) Any stroke, MI, death from any cause 7.0 (-0.9 - 14.2) * Ischemic or hemorrhagic Rupprecht HJ. Euro Heart J. 1998;19: P484 Abstract.
EpidemiologyEstimated Prevalence of Ischemic Stroke and Myocardial Infarction in North America and Europe 2000 2005 1997 Guillot F. American Heart Association; 1998 Nov. Abstract
Cirrhosis Does Not Affect the Pharmacokinetics or Pharmacodynamics of Clopidogrel • Cmax Tmax AUC Study Group (ng/mL) (hr) (range) gxhr/mL • Cirrhosis Day 1 1982.2 ± 936.4 1.0 (0.5, 2.5) 6584.5 ± 1996.8 • Controls Day 1 2192.1 ± 675.9 1.0 (0.5, 2.0) 5128.6 ± 732.1 • Cirrhosis Day 10 2453.8 ± 844.9 0.75 (0.5, 1.5) 8278.5 ± 2658.7 • Controls Day 10 2671.4 ± 1018.8 1.0 (0.5, 1.5) 6385.8 ± 1916.5 • No significant difference in mean % inhibition of aggregation at day 10 (49.2% ± 38.6 vs. 66.7% ± 7.5) • Prolongation of bleeding time was comparable at day 10(1.64 ± 0.49 vs 1.54 ± 0.87) • No dosage adjustment of clopidogrel is necessary in mild to moderate • liver impairment. Smith Ul et al. Euro Heart J. 1998;19: P490 Abstract.
CAPRIE StudyInfluence of Atherosclerotic History on Ischemic Event Rates Event Rate (%) (IS, MI, Vascular Death) PAD Only Qualifying PAD + any history* Coronary disease only Qualifying MI + any history* Cerebro- vascular disease only Qualifying IS + any history* Disease in 2 beds * Any history of atherosclerotic disease in any of the three vascular beds Cocchereri S. Euro Heart J. 1998;19: P1268 Abstract.
CAPRIE StudyInfluence of Peripheral Arterial Disease History on Ischemic Event Rates Event Rate, % (IS, MI, Vascular Death) Disease in 2 beds PAD Only Qualifying PAD group + any history* * Any history of atherosclerotic disease disease in any of the three vascular beds Cocchereri S. Euro Heart J. 1998;19: P1268 Abstract.
CAPRIE StudyInfluence of Stroke History on Ischemic Event Rates Event Rate, % (IS, MI, Vascular Death) Cerebrovascular disease only Disease in 2 beds QualifyingIS group + any history * Any history of atherosclerotic disease in any of the three vascular beds Cocchereri S. Euro Heart J. 1998;19: P1268 Abstract.
CAPRIE StudyProven Safety Profile of Clopidogrel (n=255) (n=191) (n=110) (n=104) (n=71) (n=65) (n=47) (n=34) Intracranial hemorrhage 2 GI hemorrhage 1, 2 Hospitalization due to GI2 hemorrhage GI ulcers 2 CAPRIE Steering Committee. Lancet. 1996;348:1329-1339. Data on file, Sanofi Pharmaceuticals, Inc.
RevascularizationEfficacy of Clopidogrel in PTCA • ObjectiveEvaluate efficacy and tolerance of a loading dose of clopidogrel. • Patientsn=20 (age - 56 ± 11years) with stable angina scheduled for PTCA • TreatmentASA 325 mg/day or clopidogrel 375 mg in in the morning of procedure followed by 75 mg/day maintenance. Heparin 24 hours after PTCA given to all patients. Results Mean % platelet Inhibition (5M ADP) Events • 2h 6h 8h 24h • Clopidogrel 17 ± 18% 26 ± 21%* 30 ± 26%* 20 ±10%* • ASA 5 ± 9% -2 ± 8% -3 ± 12% -8 ±19% • 1 dissection† • 3 dissections† 1 subacute occlusion * p = 0.01 † requiring stenting Conclusion: Loading doses of 375 mg clopidogrel in combination with heparin was well-tolerated and induced a rapid antiaggregatory effect that was safe and superior to aspirin. Savcic M et al. Eur Heart J. 1995;16:suppl:417 Abstract.