Download
1 / 53
530 likes | 607 Views
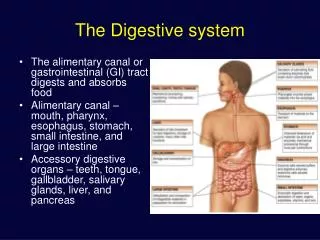
Child nutrition. The alimentary factors & developments of teeth system and development of diseases. Nykytyuk S.O.

E N D
Child nutrition. The alimentary factors & developments of teeth system and development of diseases Nykytyuk S.O
Human milk is uniquely superior for infant feeding and is species-specific; all substitute feeding options differ markedly from it. The breastfed infant is the reference or normative model against which all alternative feeding methods must be measured with regard to growth, health, development, and all other short- and long-term outcomes
Epidemiologic research shows that human milk and breastfeeding of infants provide advantages with regard to general health, growth, and development, while significantly decreasing risk for a large number of acute and chronic diseases. Research in the United States, Canada, Europe, and other developed countries, among predominantly middle-class populations, provides strong evidence that human milk feeding decreases the incidence and/or severity of diarrhea, lower respiratory infection, otitis media, bacteremia, bacterial meningitis, botulism, urinary tract infection, and necrotizing enterocolitis
There are also a number of studies that indicate possible health benefits for mothers. It has long been acknowledged that breastfeeding increases levels of oxytocin, resulting in less postpartum bleeding and more rapid uterine involution. Lactational amenorrhea causes less menstrual blood loss over the months after delivery. Recent research demonstrates that lactating women have an earlier return to prepregnant weight, delayed resumption of ovulation with increased child spacing, improved bone remineralization postpartum with reduction in hip fractures in the postmenopausal period, and reduced risk of ovarian cancer and premenopausal breast cancer. In addition to individual health benefits, breastfeeding provides significant social and economic benefits to the nation, including reduced health care costs and reduced employee absenteeism for care attributable to child illness. The significantly lower incidence of illness in the breastfed infant allows the parents more time for attention to siblings and other family duties and reduces parental absence from work and lost income
RECOMMENDED BREASTFEEDING PRACTICES • Human milk is the preferred feeding for all infants, including premature and sick newborns, with rare exceptions. The ultimate decision on feeding of the infant is the mother's. Pediatricians should provide parents with complete, current information on the benefits and methods of breastfeeding to ensure that the feeding decision is a fully informed one. When direct breastfeeding is not possible, expressed human milk, fortified when necessary for the premature infant, should be provided. Before advising against breastfeeding or recommending premature weaning, the practitioner should weigh thoughtfully the benefits of breastfeeding against the risks of not receiving human milk.
Breastfeeding should begin as soon as possible after birth, usually within the first hour. Except under special circumstances, the newborn infant should remain with the mother throughout the recovery period. Procedures that may interfere with breastfeeding or traumatize the infant should be avoided or minimized
Newborns should be nursed whenever they show signs of hunger, such as increased alertness or activity, mouthing, or rooting. Crying is a late indicator of hunger. Newborns should be nursed approximately 8 to 12 times every 24 hours until satiety, usually 10 to 15 minutes on each breast. In the early weeks after birth, nondemanding babies should be aroused to feed if 4 hours have elapsed since the last nursing
No supplements (water, glucose water, formula, and so forth) should be given to breastfeeding newborns unless a medical indication exists. With sound breastfeeding knowledge and practices, supplements rarely are needed. Supplements and pacifiers should be avoided whenever possible and, if used at all, only after breastfeeding is well established
When discharged <48 hours after delivery, all breastfeeding mothers and their newborns should be seen by a pediatrician or other knowledgeable health care practitioner when the newborn is 2 to 4 days of age. In addition to determination of infant weight and general health assessment, breastfeeding should be observed and evaluated for evidence of successful breastfeeding behavior. The infant should be assessed for jaundice, adequate hydration, and age-appropriate elimination patterns (at least six urinations per day and three to four stools per day) by 5 to 7 days of age. All newborns should be seen by 1 month of age.
Exclusive breastfeeding is ideal nutrition and sufficient to support optimal growth and development for approximately the first 6 months after birth. Infants weaned before 12 months of age should not receive cow's milk feedings but should receive iron-fortified infant formula. Gradual introduction of iron-enriched solid foods in the second half of the first year should complement the breast milk diet. It is recommended that breastfeeding continue for at least 12 months, and thereafter for as long as mutually desired.
In the first 6 months, water, juice, and other foods are generally unnecessary for breastfed infants. Vitamin D and iron may need to be given before 6 months of age in selected groups of infants (vitamin D for infants whose mothers are vitamin D-deficient or those infants not exposed to adequate sunlight; iron for those who have low iron stores or anemia). Fluoride should not be administered to infants during the first 6 months after birth, whether they are breast- or formula-fed. During the period from 6 months to 3 years of age, breastfed infants (and formula-fed infants) require fluoride supplementation only if the water supply is severely deficient in fluoride (<0.3 ppm
Breastfeeding for the first year of life with the supplementation • Breastfeeding for the first year of life with the supplementation of Vitamin D from birth and iron supplementation as ferrous sulfate drops or iron-fortified cereal after 4 months of age. Fluoride supplementation may be required after 6 months of age depending on the fluoride content of the city water supply. • Feeding of iron-fortified commercial infant formula for the first year as an alternative to breastfeeding. • Delaying the use of whole cow milk until after one year of age. Early introduction of whole cow milk protein during infancy may contribute to iron-deficiency anemia by increasing gastrointestinal blood loss. Whole cow milk has an increased renal solute load compared to infant formulas. • Reduced fat milks should be delayed until after the second year of life. Adequate fat intake is important for the developing brain and milk is usually the primary source of fat for toddlers. • Delaying the introduction of semi-solid foods until 4 to 6 months of age or until the infant demonstrates signs of developmental readiness, such as head control and ability to sit with support.
There is an agreement among healthcare professionals, infant food manufacturers and mothers that breastfeeding is the best choice for feeding infants during their first four to six months of life
There are several reasons why a mother may not breastfeed her baby: • Medical or other health reasons may prevent a mother from breastfeeding. • The baby with special requirements may not tolerate breast milk. • Some social or psychological reasons can make it more difficult to breastfeed exclusively.
Table 1. Drugs that are contraindicated during breast-feeding
Table 2. Drugs that have caused significant effects on some nursing infants and should be given to nursing mothers with caution
Table 3. Drugs of abuse that are contraindicated during breast-feeding
Common problems encountered with brest-feeding • Poor Let-Down (Milk ejection reflex) • Poor Weight Gain • Mastitis • Cracked Nipples • Jaundice From Breast- Feeding
Artificial feeding • This is the feeding of infant when he gets cow’s or buffalo’s milk or formula from first days till 4th to 6th month of his life.
Formula milks are humanized, i.e., they come very close to the composition of breast milk. • However, they are more expensive, so cow’s or buffalo’s milk are quite often used.
Other advantages of breast milk versus cow’s milk: • Breast milk is available all the time and is practically free from pathogenic bacteria. • It needs no time for preparation • It is available at the optimum temperature. • It contains antibodies as IgG and IgA and protects against certain infections such as E.Coli, cholera, polio, tetanus, measles etc. IgA antibodies prevent the microorganisms to adhere the intestinal mucosa and provide local GIT immunity.
β-lactose is called Bifidus factor, which promotes the growth of lactobacillus and helps to lower the gut pH, thus inhibiting the growth of E.Coli and yeasts. • Breast milk contains lactoferrin (an iron-binding whey protein), which inhibits bacterial growth by depriving them of iron, which is necessary for growth. • Breast milk contains cystine and tyrosine, which are not synthesized by infants but they are essential for proper growth and development. • Breast milk contains taurine that is synthesized in inadequate amounts in infants. It is important for normal differentiation of CNS.
Breast milk contains nonspecific factors of immune difence: lisozyme, macrofagocytes, neutrofiles, lymphocytes, complement system. • There are 5 times more essential fatty acids (polyunsaturated: arachidonic, docosahexacnoic, linoleic, and α-linolenic) in breasts milk than in cow’s milk. • Breast milk contains ferments (lipase, lactase) and mothers hormones. • Breast milk is ‘species specific’ and therefore allergy to breast milk is rare.
Dilution of Cow’s Milk: • If dilution of cow’s milk is required, add 1 TSF of sugar to each ounce of water (5 %) – isocaloric formula)
Advances in nutritional modifications of infant formulas • Proteins: their amount is adopted to the needs of infant’s organism. Almoust all formulas contain whey:casein ratio as 60:40 and adopted amino acid content.
Fats: long-chain polyunsaturated fatty acids are added in amounts similar to those in human milk.Infants fed these formulas or human milk have higher tissue concentrations of long-chain polyunsaturated fatty acids and reportedly have better visual acuity than do infants fed nonsupplemented formulas.
Carbohydrates: they are presented by β-lactose, sakcharose, dextrin-maltose, which improve the growth of Bifidum-bacteria. The total quantity of carbohydrates in formulas is 7.5 %
Nucleotides and their related products play key roles in many biological processes. Although nucleotides can be synthesized endogertously, they are considered "conditionally essential." Nucleotide concentrations in human milk are higher than in unsupplemented cow milk-based formulas, and studies in animals and human infants suggest that dietary nucleotides play a role in the development of the gastrointestinal and immune systems
For infants 0 to 12 months • Whey proteins:casein = 60:40 • Close to breast milk spectrum of amino acids • Contains taurine. • Milk fats – 74 % and plant fats – 26 % • Linoleic : α-linolenic ratio is optimal for absorption 9.9:1 • Osmolality is equal 270 mosm/L
The level of proteins is 2.2 % • Whey proteins:casein = 40:60 • Inriched with bifidum-bacteria • Fortified with vitamins
Biologically hydrolyzed casein and whey proteins • Biologically hydrolyzed lactose • Iron fortified (0.8 mg/100 ml) • Contains Bifidobacterium Lactis 2107/1 g • -6 : -3 = 7.9:1 • Osmolality 270 mosm/L
It doesn’t contain lactose • Only whey proteins are present, 20 % of them are amino acids • Contains nucleotides and selen • Iron and Iodine fortified • Contains taurine, inositol, L-karnitine.
For infants with • Hypergalactosaemia • Lactose intolerance • Strong allergy to cow’s milk proteins • Vegetarian babies
For premature and low-birth-weight (less than 2500 g) babies • Proteins – 2.3 % • Whey : casein ratio = 70:30 • Proteins are particly hydrolyzed (oligopeptids) • Contains lysine, cystine, tryptophan, L-histidine, and taurine. • Polyunsaturated fatty acids (arachidonic, docosahexacnoic, linoleic, and α-linolenic) are present
For ‘hungry’ babies • For infants with often regurgitation • Contains 77 % of casein • Iron, Iodine, Vit. D, A, E and C enriched.
NAN H.A.1 NAN H.A.2 For children with strong family allergy Contains 100 % of whey proteins, which are hydrolyzed to oligopeptids (80 %) and aminoacids (20 %) Alfaré Hypoallergenic elemental diet for children with malarbsorption syndrome, diarrhea, for tube feeding Contains hydrolyzed whey proteins: 80 % of oligopeptids and 20 % of aminoacids Hydrolyzed lactose Short-chain fatty acids
Sunlight as a source of vitamin D Adequate supplies of vitamin D3 can be synthesized with sufficient exposure to solar ultraviolet B radiation Melanin, clothing or sunscreens that absorb UVB will reduce cutaneous production of vitamin D3
Reasons of vitamin Ddeficiency • Environmental conditions where sunlight exposure is limited like indoor confinement or working indoors during daylight hours may reduce source of vitamin D; • Inadequate daily consumption - a lack of vitamin D, calcium and phosphorous in the diet, have trouble digesting milk products, people who are lactose intolerant;
Reasons of deficiency vitamin D • Problem of malabsorption called steatorrhea, in which the body is unable to absorb fats. The result of this problem is that Vitamin D, which is usually absorbed with fat, and calcium are poorly absorbed. • This poor absorption can be a result of digestive disorders. • Liver, kidney failure (congenital or acquired disorders) - due to tubular acidosis in which there is an increased amount of acid in the body; • Dark Pigmentation