Download
1 / 61
610 likes | 678 Views
Community Partnerships Across the Lifespan. Presenters. Richard N .Roberts Director Early Intervention Research Institute. Jennifer M. Cernoch Executive Director Family Voices. Adrienne L. Akers Senior Research Scientist Early Intervention Research Institute. Facilitator. Diane D. Behl

E N D
Community Partnerships Across the Lifespan Presenters Richard N .Roberts Director Early Intervention Research Institute Jennifer M. Cernoch Executive Director Family Voices Adrienne L. Akers Senior Research Scientist Early Intervention Research Institute Facilitator Diane D. Behl Senior Research Scientist Early Intervention Research Institute Maternal and Child Health Bureau, Federal/State Partnership Meeting, Washington, DC October 18, 2005
Click image to begin Click here to continue
What are Integrated Services? • Services are organized so families can use them easily • Efficient use of resources • Family-level strategies (e.g., care coordination) • Systems-level strategies (e.g., common application systems, coordinated service plans, shared data) • Community-based with state and federal support and continuity • Systems designed to work for all children, especially CYSHCN, across the age span
Partners in Continuous Quality Improvement Richard N .Roberts, Ph.D. Director Champions for Progress Center Early Intervention Research Institute 6580 Old Main Hill Utah State University Logan, UT 84322-6580 (435) 797-1172 Richard.Roberts@usu.edu
What is your goal/outcome to be achieved? • Can you define it? • Can you measure it?
Who else can help? • Faith-based organizations • Business community • Chambers of Commerce What help is needed? • Staffing • Financial management • Fund raising
What would a plan of action look like? • Organizational issues • Bench markers • Specific “to do’s”
How integrated are the services and supports already at your level? • Is there a council? • Do people talk to each other? • Are there formal agreements? • Do data drive the decision making? • Who is not at the table but should be?
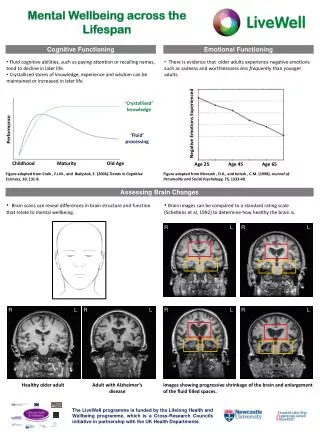
Pocatello Service Integration Matrix (April 2001 – Follow-up Data) Service Integration Goal: Coordination of Early Intervention with the Medical Home Target Population: 0-5 Part C/Part B in CDS or CSHCN Definition Children and Families Outcomes and Accountability: Referrals from local physicians to early intervention: 16% in 1999; Key: P = Prior to task force Intensity of Integration Continuum 1999 = 1999 SI level Informal Formal I = Ideal level in 1999 2001 = 2001 SI level P I 1999 2001 I P 2001 1999 1999 I P 2001 P 1999 I 2001 I P 2001 1999 P I 1999 2001 I P 1999 2001 increased to 26% in 2001. No Connection Information Sharing and Communication Cooperation and Coordination Collaboration Consolidation Integration Partners/stakeholders Shared goals/mission statement Connections b/w task force and state agencies Community task force governance and authority Service delivery system/model Financing and budgeting Information systems/data management
Building Partnerships Across the Lifespan for Children and Youth with Special Health Care Needs 2005 HRSA/MCHB Partnership Meeting Jennifer M. Cernoch Executive Director
A national grassroots organization of over 40,000 families and friends speaking on behalf of children and youth with special health care needs that provides: • Information • Education • Support • Advocacy
FV Mission & Core Principles Mission:Advocate for health care services that are family-centered, community-based, comprehensive, coordinated and culturally competent; promote the inclusion of all families as decision makers at all levels of health care; and support essential partnerships between families and professionals. • Partnership… strong family-professional partnerships improve decision-making, enhance outcomes, and assure quality. • Accountability … what families practice every day – cost effectiveness without compromising quality, in the delivery of services.
Partnerships = Family-Centered Care = Best Practice The foundation of family-centered care is the partnership between families and professionals. Based on this partnership, family-centered care: • Acknowledges the family as the constant in a child’s life. • Builds on family strengths. “Every child deserves a horizon, NOT a box” ---Mom of son with neuromuscular disorder • Supports the child/youth in learning about and participating in his/her care and decision -making.“I know you don’t understand everything I am trying to say, but I am glad you take time to listen to me” ---Teen with mental illness at transition IEP • Honors cultural diversity and family traditions. • Recognizes the importance of community-based services.
Partnerships = Family-Centered Care = Best Practice • Promotes an individual and developmental approach. “Don’t go out of the room to talk about me. Don’t tell me it won’t hurt because it does. Be honest with me … tell me the truth. Don’t think I won’t understand” --- Girl with terminal cancer • Encourages family-to-family and peer support. • Supports youth as they transition to adulthood.“Can someone teach me what to do, who will help me with my needs when my parents will no longer be here?” -- 11 year old girl with cerebral palsy • Develops policies, practices, and systems are are family-friendly and family-centered in all settings. • Celebrates successes.“They took me flying down the ski slopes. I was so excited I think I stopped breathing! I did it … Can you believe it? I DID IT! -- Boy with Bi-Lateral Amputee
Critical Components of PartnershipsNational Center on Family/Professional Partnerships • Families and/or youth are making decisions at all levels. • Families and youth are satisfied with the services that they receive.
Building Partnerships • Partner: one who shares with another or others for a mutual benefit • Essential Components: • Building trust • Actively listening & engaging – open & honest • Open to new opportunities for learning • Establishing clear expectations, roles & responsibilities • Acknowledging mutual respect for each others’ cultures, values and traditions
Partnerships Across the Lifespan Birth infant toddler preschool school-aged adolescent young adult
Why are Partnerships Important? The Reality for Families and Youth Because …. • 39.5% indicate their child’s condition impacts family’s financial situation • 28.5% indicate families stop working due to child’s condition • 24.9% indicate they cut back on work due to child’s condition • 13.5% say they spend 11+hours/wk coordinating care for their CSHCN • 5.8% say that youth are receiving services necessary to transition to adulthood MCHB/NCHS. National Survey on Children with Special Health Care Needs. 2002.
Why are Partnerships Important? • FV Survey – Your Voice Counts – families are satisfied with health services when they are partners with the primary care provider (2000) • Families rely on other families to get information – peer support is the most important source of information • Evidence-based studies show that families of CYSHCN want: • state level support that is formally organized -staffed with paid parents • increased parent/professional communication and understanding • to play an important role in educating professionals around the changes in attitudes, behaviors, practices and procedures for quality health care
Achieving Full Partnerships for All CYSHCN “We who have children with special health care needs have learned patience, joy, and resilience which comes from the lessons our children have taught us. Through them, our lives have been enriched, learning from those lessons and sharing them with those who also have devoted their lives, partnering with us in each step” --- D Feist 2010
Can I Get Some Help Around Here? A Web-Based Interagency Application Process Adrienne Akers, M.S., R.P.T. Early Intervention Research Institute Utah State University Logan, UT 84322-6580 adrienne.akers@usu.edu
System Barriers Identified by Families • Multiple assessments • Poor coordination between EI & medical home • Lack of shared data • Redundant paperwork (FICC, 1998)
Part C Baby Your Baby CSHCN Head Start Medicaid Completing paperwork is frustrating!
CSHCN Part C Baby Your Baby Head Start Medicaid Online applications simplify the process
a web-based interagency application process designed to help families apply for multiple programs & services online currently available in English & Spanish available 24/7 Utah Clicks!Universal Application System (UAS)
More children are entering the service system Federal/state mandates to organize services Federal/state budget cuts require cost efficiencies Trend toward e-Government & paperless applications Why Develop Utah Clicks?
Application Process:Client fills out agency paperwork prior to eligibility determination.--This is accomplished via Utah Clicks Eligibility Process:Agency’s intake worker determines if a client (and his/her application) meets thefinancial or serviceneed criteriato receive benefits or services from that agency.--This is not accomplished via Utah Clicks Definitions
Client needs services • Client visits Utah Clicks website: • Creates account • Answers screening questions • Selects applications • Answers application questions Client’s responses are placed on PDF forms Client receives eligible services Services Client electronically submits completed applications to agencies via Utah Clicks web site Intake workers determine final eligibility Utah Clicks Overview
Families identify application forms that they want & need & are targeted first. Families are screened in, not out. The current paper-based intake process is mirrored as closely as possible. The intake process is streamlined so that workers can focus more on helping than on paperwork. Guiding Principles of Utah Clicks
Applications CurrentlyAvailable on Utah Clicks • Baby Watch/Part C • Baby Your Baby • CHIP (in process) • CSHCN • Medicaid • WIC (Jan ’06)
94% completed Utah Clicks in one session. How long did it take to complete Utah Clicks? 0-30 minutes 52% 30-60 minutes 38% 60 minutes + 10% Data from Pilot Survey
Where did you complete the Utah Clicks? Home 64% Agency office 12% Family/Friend home 10% Work 9% Other 5% Data from Pilot Survey (cont.) 94% would recommend Utah Clicks to others !