Download
1 / 40
570 likes | 1.38k Views
Drugs for Parkinson’s disease, Alzheimer’s disease. NURS 304 Pharmacology II Dr. Nolan. Parkinson’s Disease. Parkinson’s disease progressive, degenerative CNS disease (“neurodegenerative disorder”)

E N D
Drugs for Parkinson’s disease, Alzheimer’s disease NURS 304Pharmacology II Dr. Nolan
Parkinson’s Disease • Parkinson’s disease • progressive, degenerative CNS disease (“neurodegenerative disorder”) • loss of dopamine producing cells in the substantianigra in the basal ganglia of the midbrain, an area of the brain that controls voluntary muscle movement
Parkinson’s Disease • Parkinson’s disease • presentation • initial is often “pill rolling” movements with finger and thumb • resting tremor, bradykinesia • rigidity (muscles tensed and slowed to the point of absolute rigidity) • stooped posture • gait freezing and falls • hypomimia (mask-like or reduced facial expression) • akinesia (inability to move a muscle) • micrographia • dysphagia • hypophonia
Parkinson’s Disease • Parkinson’s disease • incidence • 1.5 million in US • most > 50 y.o. • Average age of diagnosis is 58 to 62 years • 1.1 million PD patients in U.S., 76% over age of 65, mostly men • 50 to 60 thousand newly diagnosed in US each year
Parkinson’s Disease • pathophysiology • deficiency of dopamine in the basal ganglia • destruction of dopamine producing cells leads to relative decrease in dopamine (inhibitory) vs. acetylcholine (excitatory) • cause of PD is unknown • Course of disease • Progressive symptoms become less responsive to gold standard treatment with levodopa • “Wearing off” and “on/off phenomenon”
Parkinson’s Disease • treatment • Primary • increase dopaminergic stimulation by: • replacing dopamine with levodopa • giving dopamine agonist • inhibiting breakdown of CNS dopamine • Secondary • restore balance of dopamine and Ach by reducing the CNS level of ACh (anticholinergic drugs)
Anti-Parkinson’s drugs • Drug treatment • Replace dopamine • levodopa • seek to restore dopamine lost by destruction of dopamine producing cells • Stimulate dopamine receptors • bromocriptine, ropinirole, pramiprexole, rotigotine • Inhibit breakdown of CNS dopamine • selegiline, rasagiline • Increase synaptic levels of CNS dopamine • amantadine
Anti-Parkinson’s drugs • Dopaminergic drugs • levodopa • dopamine does not cross the BBB, so we give levodopa • drug of choice for primary treatment of Parkinson’s • dosed orally • improves all symptoms and QOL • very quick improvement of bradykinesia (“off time”) • dosed 3-5 times per day • half life is 1-3 hours
Anti-Parkinson’s drugs • Dopaminergic drugs • levodopa cont’d • converted in the CNS to dopamine by amino acid decarboxylase (AADC) • converted dopamine is then stored in presynaptic DA neurons • as fewer of these are available, levodopa becomes less effective and shorter acting (“off time”) • initiation of levodopa in younger patients may be delayed to avoid levodopa induced dyskinesias and “wearing off”
Anti-Parkinson’s drugs • Dopaminergic drugs • levodopa cont’d • side effects • ↑ IOP, activation of malignant melanoma • dyskinesias, anorexia, N/V, confusion, dizziness, dry mouth • ~50% of patients experience levodopa induced dyskinesias by year 5 of therapy. 80% by year 10. • Young onset PD may benefit from “levodopa sparing” strategy to avoid years of considerable dyskinesias
Anti-Parkinson’s drugs • Dopaminergic drugs • levodopa cont’d • End of dose wearing off • levodopa duration of action becomes shorter • higher doses or more frequent dosing leads to profound dyskinesias • eventually all PD patients experience significant “off time” that can be hours per day • Levodopa induced dyskinesias • the exaggerated and involuntary movements seen in PD patients is actually the effects of levodopa • All PD patients are eventually faced with levodopa induced dyskinesias • probably due to non-physiologic pulsatile dopaminergic stimulation
Anti-Parkinson’s drugs • Dopaminergic drugs • levodopa cont’d • bioavailability of levodopa can be increased by reducing it’s peripheral conversion to dopamine (which cannot cross the BBB and is responsible for many of levodopa’s side effects) • Agents that decrease the enzymatic metabolism of levodopa: • AADC inhibitors • COMT inhibitors
Anti-Parkinson’s drugs • inhibitors of levodopa metabolism • COMT inhibitors • inhibits action of peripheral COMT, which metabolizes levodopa (10% of metabolism via COMT) • enhance the bioavailability of levodopa • tolcapone crosses the BBB so also inhibits CNS metabolism of DA by COMT (minor contribution) • are given ONLY WITH levodopa • levodopa dose must be ↓when used with a COMT inhibitor
Anti-Parkinson’s drugs • inhibitors of levodopa metabolism • COMT inhibitors cont’d • entacapone (Comtan®), tolcapone (Tasmar®) • side effects • entacapone (Comtan®) • confusion, dizziness, sedation, hallucinations, N/V • tolcapone (Tasmar®) • diarrhea, liver failure (BBW) - LFT q 2 wks x 1 year
Anti-Parkinson’s drugs • inhibitors of dopamine metabolism • AADC inhibitor • Amino acid decarboxylase responsible for converting levodopa to dopamine in periphery and in CNS • Carbidopa inhibits AADC, so levodopa is not broken down peripherally before it can pass the BBB • allows for 70% smaller doses of levodopa • Carbidopa does not cross BBB, so does not interfere with AADC conversion of levodopa to dopamine in CNS • fixed dose combination with levodopa • levodopa/carbidopa (Sinemet) • ONLY given along with levodopa
Anti-Parkinson’s drugs • dopamine receptor agonists • bromocriptine, pramiprexole (Mirapex®), ropinirole (Requip®) • mechanism of action • directly stimulate postsynaptic DA receptors • useful in early and late stage PD • early use can delay start of levodopa • more side effects in elderly, so never given as first line therapy • Sometimes used as initial therapy in younger PD patients to delay the development of dyskinesias 2° levodopa use • These drugs are also used in RLS
Anti-Parkinson’s drugs • dopamine receptor agonists • common side effects • GI - nausea, dyspepsia, anorexia • CNS - somnolence, dizziness, visual changes • hypotension • malaise • headache • uncommon side effects • compulsive (pathological) gambling • Requip (ropinirole) most often implicated • hallucinations, syncope
Anti-Parkinson’s drugs • dopamine receptor agonists • apomorphine (Apokyn) • SQ injection for acute, intermittent treatment of “off episodes” (hypomobility) • side effects include N/V, hypotension • given as 0.3mL (3 mg) or 0.6mL (6 mg) dose, up to 5x per day • only 1 dose per episode, efficacy of 2nd dose not established • Test Dose (in office) • pt in “off” state s/b given 0.2mL (2mg) dose • closely monitor supine and standing BP predose and 20, 40, 60 min post dose • pts with clinically significant orthostatic hypotension are not candidates for Apokyn® • if tolerated, dose is 0.2mL, ↑ by 0.1mL q few days in needed • antiemetic prophylaxis! • severe nausea and vomiting will occur without antiemetic on board • trimethobenzamide usually used, 300mg TID starting 3 days prior
Anti-Parkinson’s drugs • inhibitors of dopamine metabolism • MAO-B inhibitors • mechanism of action • MAO-A breaks down tyramine, NE, epinephrine, and serotonin • MAO-B breaks down dopamine • MAO-B selective inhibitors increase CNS dopamine and don’t fewer risks than MAO-A inhibitors • Selectivity lost at doses > 10mg! • act in CNS, NOT in the periphery (like COMT inhibitors) • selegiline (Eldepryl®) • irreversible MAO-B inhibitor • actions may last months, until more MAO synthesized in CNS
Anti-Parkinson’s drugs • inhibitors of dopamine metabolism • MAO-B inhibitors cont’d • selegiline (Eldepryl®) cont’d • probably drug of choice for early PD monotherapy • in advanced disease, added to levodopa to enhance it’s effect • rasagiline (Azilect®) • irreversible MAO inhibitor, not selective for MAO-B • same indications/use as selegiline • watch for all the usual MAOI interactions (food and drugs)
Anti-Parkinson’s drugs • Dopaminergic drugs • dopamine reuptake inhibitors • mechanism of action • stimulate presynaptic release of DA • inhibit presynaptic reuptake of DA • amantadine (Symmetrel®) • starts working within a week • stops working after a couple months of continuous use • often given in 1-2 week periods when symptoms worsen • not as effective as levodopa • more effective than anticholinergics
Anti-Parkinson’s drugs • Anticholinergic drugs • mechanism of action • reduce the relative excess of acetylcholine vs. dopamine • use • effective for tremor, salivation, and spasticity • not effective for bradykinesia • benztropine (Cogentin®), trihexyphenidyl, diphenhydramine (Benedryl®) • all the usual anticholinergic side effect apply
Parkinson’s Disease • Drugs than can make PD worse • antipsychotics (typical and atypical) • antiemetics • promethazine (Phenergan), metoclopramide (Reglan), prochlorperazine (Compazine) • dopamine depleting drugs • reserpine, methyldopa
Parkinson’s Disease • Non motor symptoms of PD • common and debilitating (60% of PD patients have non-motor symptoms as well) • Autonomic • orthostatic hypotension • impotence • urinary frequency • GI motility problems (constipation) • cold limbs and drenching sweats • Psychiatric/Cognitive • dementia (can exceed 40% incidence) • sleep disorders • depression, anxiety • drug induced psychosis
Alzheimer’s Disease • incurable, progressive, degenerative, terminal disease • most common dementia • etiology • protein plaques and “tangles” in brain (beta amyloid protein plaques in the empty spaces between neurons, tau protein deposits inside neurons) • presentation • early sign is difficulty acquiring new memories • disease progression: confusion, irritability, aggression, long term memory loss, language problems, withdrawal • eventual death as bodily functions decline • average time from diagnosis to death: ~7 years • usually from pneumonia, infection • incidence • 1 in 8 people > 65 y.o. • about 1 in 2 > 85 y.o. • familial risk: 2-3x more likely to have alzheimer’s if parent or sibling does
Alzheimer’s Disease • treatments • no cure, no treatment to alter progression of disease • acetylcholinesterase inhibitors may help with symptoms for a short time • based on the loss of cholinergic neurons by plaques • donepezil (Aricept®), galantamine (Razadyne®), rivastigmine (Exelon® tabs and patch) • MOA • inhibit the enzyme acetylcholinesterase, which is responsible for breaking acetylcholine down • results in higher CNS levels of acetylcholine
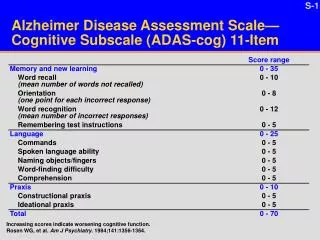
Efficacy of Aricept Many of the studies show statistical significance, but little, if any, clinical significance. • ADAS (Alzheimer Disability Assessment Scale) used to evaluate attention, memory, orientation, language and speech: a change of 4 points is considered clinically significant. • CIBIC (Clinician based Impression of Change): any change is considered clinically significant. • MMSE: a change of 3 points is considered clinically significant.
Studies on Aricept Most of the studies are short term (almost all less than 1 year and mostly 6 months) • There is little guidance of what to do with these meds beyond the 612 month mark with real patients. • Most of the trials exclude patients with significant comorbid conditions. • Most demented patients have lots of complex medical issues
DonezepilEfficacy Data • Lancet June 26, 2004 Courtney et al • 565 community resident patients with mild- moderate Alzheimer’s Disease (AD) were blindly randomized to 5mg or 10mg of donepezil or placebo and were followed for 3 years.
Lancet June 26, 2004 • Results: • Donepezil group averaged 0.8 MMSE points better (p<0.0001) • (remember: 3 or more points to be clinically significant) • No benefit in donepezil group compared with placebo in institutionalization (42% vs 44% at 3 years p=0.4) or in progression of disability (58% vs 59% at 3 years p=0.4) • No benefit in behavioral or psychological symptoms, caregiver psychopathology, formal care costs, adverse events or deaths.
DonezepilEfficacy data • Cochrane Database Syst Rev 2006Jan25 • Searched for all unconfounded,double blind randomized controlled trials in which treatment with donepezil was compared with placebo for patients with mild, moderate and severe dementia (AD). • 24 trials involving 5272 patients were evaluated
Cochrane Database Syst Rev2006Jan25 • Results: • ADAS scale for cognition: 2.01 pts better for 5mg vs placebo (p<0.00001) and 2.8 pts better for 10mg vs placebo (p<0.00001) • (remember 4 or more points to be clinically significant) • Some improvement in global clinical state in 5mg and 10mg compared with placebo in number of patients showing improvement or no change (OR= 2.18 {5mg} and OR=2.38{10mg}.
Adverse Events • Prescriber’s Letter look at the literature indicates NNHarm= 12 with cholinesterase inhibitor and NNT = 42 to get a significant positive effect. • Cochrane Rev 2006: withdrawal rates 0% to 57% in donepezil groups and 0%-20% in placebo groups. • GI side effects are most common, improve with time, diminished with lower doses and taking with food. Some suggest prescribing an anti-nausea drug.
Arch Intern Med May 11, 2009 • Results: • Hospital visits for syncope: • 31.5 (cholinesterase inhibitor) vs 18.6 (placebo) events/1000 person-years; HR=1.76 • Hospital visits for bradycardia: • 6.9 (C.I.) vs 4.4 (placebo) events/1000 person-years; HR=1.69. • Permanent pacemaker insertion: • 4.7(C.I.) vs 3.3 (placebo) per 1000 person-years; HR=1.49. • Hip fracture: • 22.4(C.I.) vs 19.8 (placebo) events per 1000 person-years; HR= 1.18