Download
1 / 24
770 likes | 3.13k Views
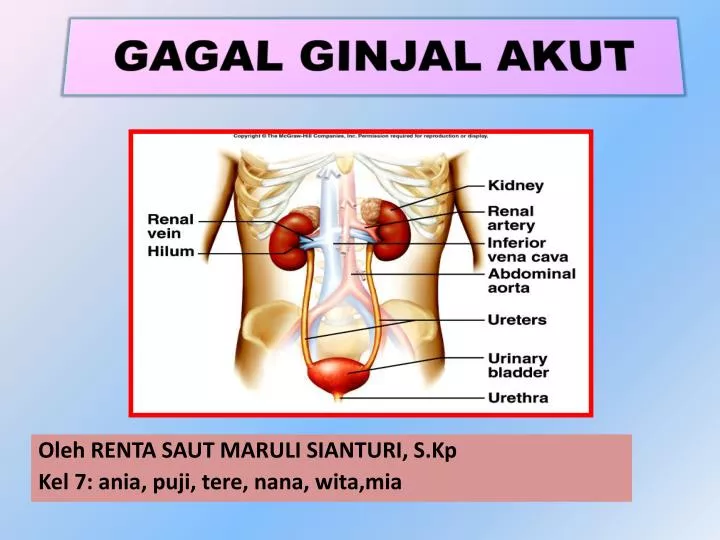
GAGAL GINJAL AKUT. Oleh RENTA SAUT MARULI SIANTURI, S.Kp Kel 7: ania, puji, tere, nana, wita,mia. Defenition.

E N D
GAGAL GINJAL AKUT Oleh RENTA SAUT MARULI SIANTURI, S.Kp Kel 7: ania, puji, tere, nana, wita,mia
Defenition • Acute renal failure is a rapid decrease in renal function over days to weeks, causing an accumulation of nitrogenous products in the blood (azotemia). (www.kidney fun.org /American Kidney ) • Acute renal failure (also called acute kidney injury) means that your kidneys have suddenly stopped working • Acute • sudden onset • rapid reduction in urine output • Usually reversible • Tubular cell death and regeneration
Causes of ARF • Pre-renal = • vomiting, diarrhea, poor fluid intake, fever, use of diuretics, and heart failure • cardiac failure, liver dysfunction, or septic shock • Intrinsic • Interstitial nephritis, acute glomerulonephritis, tubular necrosis, ischemia, toxins • Post-renal = • prostatic hypertrophy, cancer of the prostate or cervix, or retroperitoneal disorders • neurogenic bladder • bilateral renal calculi, papillary necrosis, coagulated blood, bladder carcinoma, and fungus
Fase klinis GGA • Initiating phase adanya pencetus s/d timbul gejala oliguria 2. Oliguria (Vol. Urin <400 cc/hari)1-2 minggu peningkatan BUN, creatinin, as. Organik,as. Organik,as. Urat, magnesium, potasium. Problem • retensi cairan • Hiperkalemi, hipermagnesia • Asidosis metabolik • Resti infeksi • Perdarahan saluran cerna • Perubahan nutrisi • Resti drug toxicity
3. Diuresis : “self limiting diuresis” (1-2 mgg); output urin 1-3 L/hari Problem • defisit volume cairan tubuh • hipokalemia • alkalosis metabolik 4. Pemulihan: GFR normal (6-12 bln)/ kronik Problem • Pengetahuan episode ARF • follow-up care • Pencegahan episode berulang
What are the symptoms? • Symptoms of acute renal failure may include: • Little or no urine when you urinate. • Swelling, especially in your legs and feet. • Not feeling like eating. • Nausea and vomiting. • Feeling confused, anxious and restless, or sleepy. • Pain in the back just below the rib cage. This is called flank pain. • Some people may not have any symptoms. • weakness, seizures, confusion, and coma; asterixis and hyperreflexia may be present on examination. Chest pain (typically worse with inspiration or when recumbent), a pericardial friction rub, and findings of pericardial tamponade may occur if uremic pericarditis is present. Fluid accumulation in the lungs may cause dyspnea and crackles on auscultation.
Assesment • HISTORY: • Take note of the following findings during the physical examination: • Hypotension • Volume contraction • Congestive heart failure • Nephrotoxic drug ingestion • History of trauma or unaccustomed exertion • Blood loss or transfusions • Evidence of connective tissue disorders or autoimmune diseases • Exposure to toxic substances, such as ethyl alcohol or ethylene glycol • Exposure to mercury vapors, lead, cadmium, or other heavy metals, which can be encountered in welders and miners
People with the following comorbid conditions are at a higher risk for developing ARF: • Hypertension • Congestive cardiac failure • Diabetes • Multiple myeloma • Chronic infection • Myeloproliferative disorder Orang dengan riwayat adanya penyakit pada ginjal, spt glomerulonefritis, hiperplasi prostat, etc
Physical Assesment • Skin • Petechiae, purpura, ecchymosis, and livedo reticularis provide clues to inflammatory and vascular causes of AK • Infectious diseases, thrombotic thrombocytopenic purpura (TTP), disseminated intravascular coagulation (DIC), and embolic phenomena can produce typical cutaneous changes. • Eyes • Evidence of uveitis may indicate interstitial nephritis and necrotizing vasculitis. • Ocular palsy may indicate ethylene glycol poisoning or necrotizing vasculitis. • Findings suggestive of severe hypertension, atheroembolic disease, and endocarditis may be observed on careful examination of the eyes.
Cardiovascular system • The most important part of the physical examination is the assessment of cardiovascular and volume status. • The physical examination must include pulse rate and blood pressure recordings measured in both the supine position and the standing position; close inspection of the jugular venous pulse; careful examination of the heart, lungs, skin turgor, and mucous membranes; and assessment for the presence of peripheral edema. • In hospitalized patients, accurate daily records of fluid intake and urine output and daily measurements of patient weight are important. • Blood pressure recordings can be important diagnostic tools. • Hypovolemia leads to hypotension; however, hypotension may not necessarily indicate hypovolemia. • Severe congestive cardiac failure (CHF) may also cause hypotension. Although patients with CHF may have low blood pressure, volume expansion is present and effective renal perfusion is poor, which can result in AKI. • Severe hypertension with renal failure suggests renovascular disease, glomerulonephritis, vasculitis, or atheroembolic disease.
Pemeriksaan laboratorium • 1. Darah : ureum, kreatinin, elektrolit, serta osmolaritas.2. Urin : ureum, kreatinin, elektrolit, osmolaritas, dan berat jenis.3. Kenaikan sisa metabolisme proteinureum kreatinin dan asam urat.4. Gangguan keseimbangan asam basa : asidosis metabolik.5. Gangguan keseimbangan elektrolit : hiperkalemia, hipernatremia atau hiponatremia, hipokalsemia dan hiperfosfatemia.6. Volume urine biasanya kurang dari 400 ml/24 jam yang terjadi dalam 24 jam setelah ginjal rusak.7. Warna urine : kotor, sedimen kecoklatan menunjukan adanya darah, Hb, Mioglobin, porfirin.8. Berat jenis urine : kurang dari 1,020 menunjukan penyakit ginjal, contoh : glomerulonefritis, piolonefritis dengan kehilangankemampuan untuk memekatkan; menetap pada 1,010menunjukan kerusakan ginjal berat.9. PH. Urine : lebih dari 7 ditemukan pada ISK., nekrosis tubular ginjal, dan gagal ginjal kronik.10. Osmolaritas urine : kurang dari 350 mOsm/kg menunjukan kerusakan ginjal, dan ratio urine/serum sering 1:1.
11. Klierens kreatinin urine (CCT): mungkin secara bermakna menurun sebelum BUN dan kreatinin serum menunjukan peningkatan bermakna.12. Natrium Urine : Biasanya menurun tetapi dapat lebih dari 40 mEq/L bila ginjal tidak mampu mengabsorbsi natrium.13. Bikarbonat urine : Meningkat bila ada asidosis metabolik.14. SDM urine : mungkin ada karena infeksi, batu, trauma, tumor, atau peningkatan GF.15. Protein : protenuria derajat tinggi (3-4+) sangat menunjukan kerusakan glomerulus bila SDM dan warna tambahan juga ada. Proteinuria derajat rendah (1-2+) dan SDM menunjukan infeksi atau nefritis interstisial. Pada NTA biasanya ada proteinuria minimal.16. Warna tambahan : Biasanya tanpa penyakit ginjal ataui infeksi. Warna tambahan selular dengan pigmen kecoklatan dan sejumlah sel epitel tubular ginjal terdiagnostik pada NTA. Tambahan warna merah diduga nefritis glomular.
Pemeriksaan darah 1. Hb. : menurun pada adanya anemia.2. Sel Darah Merah : Sering menurun mengikuti peningkatan kerapuhan/penurunan hidup.3. PH : Asidosis metabolik (kurang dari 7,2) dapat terjadi karena penurunan kemampuan ginjal untuk mengeksresikan hidrogen dan hasil akhir metabolisme.4. BUN/Kreatinin : biasanya meningkat pada proporsi ratio 10:15. Osmolaritas serum : lebih beras dari 285 mOsm/kg; sering sama dengan urine.6. Kalium : meningkat sehubungan dengan retensi seiring dengan perpindahan selular ( asidosis) atau pengeluaran jaringan (hemolisis sel darah merah).7. Natrium : Biasanya meningkat tetapi dengan bervariasi.8. Ph; kalium, dan bikarbonat menurun.9. Klorida, fosfat dan magnesium meningkat.10. Protein : penurunan pada kadar serum dapat menunjukan kehilangan protein melalui urine, perpindahan cairan, penurunan pemasukan, dan penurunan sintesis,karena kekurangan asam amino esensial11. CT.Scan12. MRI13. EKG mungkin abnormal menunjukan ketidakseimbangan elektrolit dan asam/basa.
Komplikasi Possible Complications • Chronic (long-term) kidney failure • Damage to the heart or nervous system • End-stage kidney disease • High blood pressure • Loss of blood in the intestines
Acute Renal Failure Management • Make/think about the diagnosis • Treat life threatening conditions • Hipoperfusi renal: - Normovolemia : resusitasi cairan CVP 12 - Normotensi: norepinefrin - furosemid • Identify the cause if possible • Hypovolemia • Toxic agents (drugs, myoglobin) • Obstruction • Treat reversible elements • Hydrate • Remove drug • Relieve obstruction
Nursing Diagnosis • 1. Perubahan kelebihan volume cairan b/d gagal ginjal dengan kelebihan air.2. Resiko tinggi terhadap menurunnya curah jantung berhubungan dengan ketidakseimbangan cairandan elektrolit, gangguan frekuensi, irama, konduksi jantung, akumulasi/penumpukan urea toksin, kalsifikasi jaringan lunak.3. Gangguan pemenuhan nutrisi kurang dari kebutuhan tubuh berhubungan dengan katabolisme protein4. Kelelahan berhubungan dengan penurunan produksi energi metabolik/pembatasan diet, anemia.5. Resiko tinggi terhadap infeksi b/d depresi pertahanan imunologi.6. Resiko tinggi terhadap kekurangan volume cairan b/d kehilangan cairan berlebihan.7. Kurang pengetahuan tentang kondisi,prognosis dan kebutuhan pengobatan b/d kurang mengingat.