Download
1 / 46
500 likes | 739 Views
Cost Driver Analysis. Christoff Raath Health Monitor Co. 10 July 2006. National Health Monitor. Industry-wide scenario modeling tool Annual statutory returns Extended through detailed scheme data All registered schemes and options Database 2002 onwards. Medical Scheme Income Statement.

E N D
Cost Driver Analysis Christoff Raath Health Monitor Co. 10 July 2006
National Health Monitor • Industry-wide scenario modeling tool • Annual statutory returns • Extended through detailed scheme data • All registered schemes and options • Database 2002 onwards
MSA Risk Contri-bution NonHCExp Reserves
Claimed MSA Unused Risk Contri-bution NonHCExp Reserves
GP • Specialist • Medicine • Dental • Radiology • Pathology • Hospital • Other MSA Risk Contri-bution NonHCExp Reserves
MSA Risk Admin Contri-bution Broker fees NonHCExp Managed Care Other Reserves
MSA Risk Contri-bution NonHCExp Investment and other income Reserves
Contribution Levels Solvency Level Type of Scheme Contributions per member per month over 2002-2004
Scheme Distribution Number of members in different types of schemes
Composition of Contributions Contributions per member per month
Contribution Increases Broken Down Increases per year 13.8% 10.0% 6.2%
Contribution Increases Broken Down Annualised increases 2002-2004 per type of scheme 10.8% 10.0% 9.4%
Contribution Increases Broken Down Annualised increases 2002-2004 per solvency level 14.7% 10.0% 10.1%
Contribution Increases • Benefits 6.2% • Reserve building 2.3% • Non healthcare exp 1.3% • MSA 1.3% • Investment & other income (-0.9%)
Real Contribution Increases Increases over CPI per year 6.7% 5.8% 4.9%
Real Contribution Increases • Benefits 3.1% • Reserve building 1.7% • Non healthcare exp 0.7% • MSA 0.8% • Investment & other income (-0.7%)
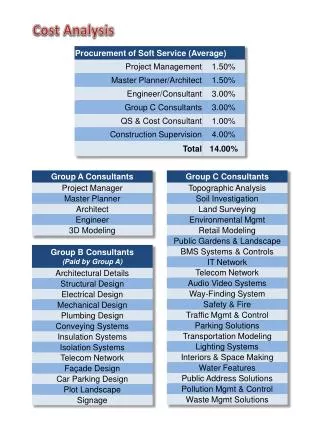
Expenses • Administration • Managed health care • Commission • Other
Expense Composition (Rands) Expenses per member per month, average over 2002-2004
Expenses Increases (%) Annualised increases in expenses over 2002-2004
Surpluses Generated Surplus per member per month over 2002-2004
Increase in Surpluses Annualised increase in pmpm surpluses generated 2002-2004
Risk Benefits Distribution of risk benefits, 2002-2004
Benefits (Rands) Average spent per member per month over 2002-2004
Benefits (%increase) Annualised increases in risk benefits over 2002-2004
Benefits (%increase) Annualised increases in risk benefits over 2002-2004
Conclusions • Risk benefits • Hospitalisation • Benefit design • Demographic changes insignificant • Surplus generation • Scheme behaviour influenced by • Solvency requirements • Prescribed minimum benefits
Benefits (weighted %increase) Weighted annualised increases in risk benefits over 2002-2004
Hospital cost analysis:2003-2005 Rajesh Patel BHF
Objectives • Presentation limited to results of: • Effect of Hospital Network on cost variability • Effect of alternate re-imbursement models
Data bias • 2006 BHF requested 2 data sets for analysis • Event cost • Aggregated data to evaluate population risk & utilisation • 1 administrator reponded • Part of 1 data set received • Results presented are therefore biased
Method • Dependent variable: Hospital cost 2003-5 • GLM1: Main effects • GLM2: with interaction
GLM1 Treatment year Hospital* Hospital network Physician practice type Basket of Procedures Payment type Age bands Region GLM2 Hospital* Physician practice type Basket of Procedures Payment type Age bands Region Treatment year X Hospital network Stratified by
Results • Model was strong (had power) • All variables used explained data variability • P < 0.0001
Y intercept = R12937 • Essential data for negotiation • Explain variance
Reason for higher cost of some networks • Lack of billing standardisation • Differences in interpretation • chargable vs non chargable • Problem perpetuated by competition commissioner ruling • Unregulated access to technology • Practitioner driven but clinic funded • E.g. disposable vs non disposable • Unregulated prices – non MCC items
What is your experience/perception about re-imbursement (per diems) and FFS effect on hospital cost per admission? • FFS is more costly • Per Diem is more costly • Don’t know • No vested interest, prefer to abstain
Per Diems • Entrenched in US • With a number of funds it’s more costly than FFS • They cannot move away from it • Investers / Network Board of Directors not likely to approve a lower fee structure unless guarantees of volumes • For profit entities • With cost shifting, there is a premium to be paid • Per diem cost will therefore almost always be higher than FFS in the SA environment
45% 55% • Good pricing and negotiation by network and funders • Effect of outlier threshold – study the contract • How is outlier threshold determined?
If “Yes” to last question • Are you willing to share data in support of your answer? • Yes • No • Don’t know need to consult • Would you like to see per diems in current code structure removed? • Yes • No
Conclusions • Urgent need for billing standardisation • Need to engage a willing HASA • No discussion of fees! – CC rules! • Effect of network on hospitalisation cost (for this data set) is consistant regardless of type/dimension of analysis • Tested recent claims made by private hospital industry • Is per diems the ideal alternate reimbursement method? • Recent contracts -not renewed or cancelled