Download

1 / 29
290 likes | 454 Views
EUS: the nonmucosal lesion. GIST (stromal tumor) Lymphoma (MALT) Carcinoid Extrinsic compression Submucosal metastasis Cystic lesion. T: Depth of Tumor Invasion. T1m (mucosa) Layers 1,2 T1sm (submucosa) Layer 3 T2 (muscularis propria) Layer 4 T3 (adventitia, serosa) Layer 5

E N D
EUS: the nonmucosal lesion • GIST (stromal tumor) • Lymphoma (MALT) • Carcinoid • Extrinsic compression • Submucosal metastasis • Cystic lesion
T: Depth of Tumor Invasion • T1m (mucosa) Layers 1,2 • T1sm (submucosa) Layer 3 • T2 (muscularis propria) Layer 4 • T3 (adventitia, serosa) Layer 5 • T4 (adjacent structure) Adjacent structure AJCC EUS abnormality
Impact on Esophagus Cancer One stop pre-op shop • Management: • superficial (T1N0): local therapy or surgery • locally invasive (T1-3, N1): chemo/RT + surgery • advanced(T4)/metastat/celiac: palliative
Accurate loco-regional staging Esophageal cancer • T = Depth of tumor invasion (85%) • N = Regional nodes (75%) • M = Distant mets (incl. celiac axis) • Limited utility after chemoradiation
EUS vs. CT for celiac nodes surg path (+) EUS/ FNA + test pos test # sens * EUS: 2 false neg, 2 failed due to intervening tumor Reed CE et al. Ann Thorac Surg 1999;67:319-21
EUS adds value in gastric CA • Primary lesion (T stage) • Adenopathy (N stage) • Celiac axis • Liver • Splenic hilum • Gastrohepatic ligament • Ascites
EUS FNA Technique • Outpatient procedure • Conscious sedation • 15-20 minutes • 22-25 gauge needle • Requires training • Morbidity < 0.5% • Cost EGD
EUS troubleshoots the pancreatic mass (NPV) • 32,180 diagnoses/31,800 deaths in 2005 • 75% 1 year survival, 4% 5YS • Increased use of cross-sectional imaging • Indiscriminant use tumor markers • Holy grail is early detection • But what about reassurance (NPV)
Occult Pancreatic Cancer • Back pain, wt. loss, jaundice, steatorrhea • Decompensated chronic pancreatitis • Unexplained pancreatitis • New onset hyperglycemia • Incidental pancreatic cysts Robbins, Hoffman: A Cautionary Tale in Pancreatic Cancer; Endoscopy, 2004
T-Stage Accuracy by Tumor Size EUS vs. Spiral CT Overall Legmann 1998
EUS vs. CT for celiac nodes surg path (+) EUS/ FNA + test pos test # sens * EUS: 2 false neg, 2 failed due to intervening tumor Reed CE et al. Ann Thorac Surg 1999;67:319-21
EUS adds value in gastric CA • Primary lesion (T stage) • Adenopathy (N stage) • Celiac axis • Liver • Splenic hilum • Gastrohepatic ligament • Ascites
EUS FNA Technique • Outpatient procedure • Conscious sedation • 15-20 minutes • 22-25 gauge needle • Requires training • Morbidity < 0.5% • Cost EGD
EUS troubleshoots the pancreatic mass (NPV) • 32,180 diagnoses/31,800 deaths in 2005 • 75% 1 year survival, 4% 5YS • Increased use of cross-sectional imaging • Indiscriminant use tumor markers • Holy grail is early detection • But what about reassurance (NPV)
Occult Pancreatic Cancer • Back pain, wt. loss, jaundice, steatorrhea • Decompensated chronic pancreatitis • Unexplained pancreatitis • New onset hyperglycemia • Incidental pancreatic cysts Robbins, Hoffman: A Cautionary Tale in Pancreatic Cancer; Endoscopy, 2004
T-Stage Accuracy by Tumor Size EUS vs. Spiral CT Overall Legmann 1998
EUS vs. Helical CTPancreatic cancer Resectability Vasc invasion EUS CT EUS CT EUS = CT EUS > CT *Hunt and Faigel, GIE 2002;55:232
EUS obviates need for further testing • Retrospective review (1999-2003), n=693 • Fullness, wt loss, CBD stricture, CA 19-9 • 135 had completely normal pancreas • Mean follow-up 25 months • 16 had repeat CT scan at 6 months • Negative predictive value: 100% (95% CI 98.2-100%) • Low prevalence of pancreatic cancer *Klapman et al, AJG, 2005
Celiac Plexus Neurolysis Minimizes: - Back pain - Retro bleeds - Infection - Paralysis
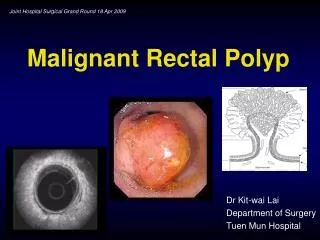
Rectal Cancer • Local recurrence after “curative” surgery is common (30-50%) • Predicted by histology, T, N stage • Adjuvant therapy: T3-4 or any N stage • Neoadjuvant: less toxicity, better local control* • How to optimally select patients for multi-modality treatment? *Swedish Rectal Cancer Trial, NEJM (1997)
EUS: More accurate than CT, MRI Author N EUST EUSN CTT CTN MRIT MRIN Rifkin (1989) 102 72% 72% 53% 71% Thaler (1994) 37 88% 80% 82% 60% Meyen (1995) 21 100% 80% Blomqvist (04) 49 60% 53% 65% 48% Bianchi (2006) 49 70% 63% 43% 64% Systematic Review Kwok (2000) 4,897 93% 71% 78% 52% 86% 65%
NCI GuidelinesRectal cancer staging “Preoperative staging procedures include digital examination, CT or MRI, endoscopy with biopsy, and EUS. EUS is an accurate method of evaluating tumor stage (up to 95% accuracy) and the status of the perirectal nodes (up to 74% accuracy).” www.cancer.gov
EUS-FNA is safe • Perforation = 0.03% (EGD) • Infection = isolated reports • Higher for cystic lesions (esp. mediastinum) • Pancreatitis = 0-2% • Bleeding = 1% • Bile peritonitis from gall bladder FNA • Celiac block = 4% diarrhea, one abscess ASGE Guidelines (2005)
EUS in the Next Decade • Strength in sampling lymph nodes • Trend towards minimally invasive resection • Molecular diagnostics, prognostics • Boutique procedure • Competition with automated imaging (CT) • Limited expert availability • Therapeutics • Injection, ablation, endosurgical applications
Therapeutic EUS • Injection • Immune therapy • Viral therapy • Gene therapy • Neurolysis • Therapeutic fistula formation • Implantation – radiation seeds • Tumor ablation • heat • cold Cancer treatment
Early Cancer Detection The Toolbox • Chromoendoscopy • High resolution endoscopy (HRE) • Narrow band imaging (NBI) • Autoflorescence (AFI) • Confocal microscopy • Endocytoscopy (ECS) • Optical coherence tomography (OCT)
Early Cancer Detection The Applications • Barrett’s esophagus • Early gastric cancer • Dysplasia in IBD • Colonic polyp detection