Download
1 / 51
530 likes | 553 Views
Caries Risk Assessment and its interaction with Preventive and Restorative Protocols. Richard Ehrlich DDS www.elmtreedental.com dre@elmtreedental.com. Introduction. Caries Risk is used by most general dentists daily, usually on an intuitive level.

E N D
Caries Risk Assessmentand its interaction with Preventive and Restorative Protocols Richard Ehrlich DDS www.elmtreedental.com dre@elmtreedental.com
Introduction Caries Risk is used by most general dentists daily, usually on an intuitive level. The first part of this presentation will attempt to help quantify this, and the second part will use this information for more systematic preventive, diagnostic and restorative protocols.
Applications of Caries Risk Assessment Caries Risk Assessment assists in predicting and diagnosing this type of case- Should you observe this? Or does it conceal this?
Applications of Caries Risk Assessment Caries Risk Assessment assists in predicting and diagnosing this type of case- Should you replace these restorations or observe them?
Overview of Caries Risk Assessment (CRA) • Caries Risk Assessment (CRA) is a simple, quick method for assigning a number to an individual’s risk for decay. • Using this data, custom preventive and restorative programs can be used, with more reliance on evidence-based dentistry and less on intuition and experience alone. • This simplified version is based on practical application of the U of T Caries Risk Assessment in actual clinical practice in a preventive-oriented dental office.
Categories for Simplified CRA These are all given numerical scores: • Existing Decay • Previous Decay • Root Caries • Fluoride Exposure • Diet Factors • Oral Hygiene • Additional Tests • S.mutans and Lactobacillus • Saliva Flow
Existing Decay No Decay = 0 Some early Pit and Fissure Decay = 0.5 1-2 Existing Lesions =1 >2 Lesions =2 Categories for Simplified CRA
Previous Decay No Decay = 0 Some early Pit and Fissure Decay = 0.5 Interproximal Posterior Decay =1 Anterior or Smooth Surface Decay =2 Categories for Simplified CRA
Existing Decay Previous Decay Root Caries Ratio of exposed root surfaces to decay <25% of root surfaces decayed = 0 25%-50% of surfaces decayed =1 >50% of surfaces decayed =2 Categories for Simplified CRA
Existing Decay Previous Decay Root Caries Fluoride Exposure Using Fluoride Toothpaste BID = 0 Using Fluoride Toothpaste once daily = 1 Not using Fluoride Toothpaste or Rinse = 2 Categories for Simplified CRA
Categories for Simplified CRA • Existing Decay • Previous Decay • Root Caries • Fluoride Exposure • Diet Factors
Diet Factors: • The Diet Questionnaire is presented. • Total sugar exposures are totaled, and divided by 3 for the Caries Index Diet Score
Diet Questionnaire: • Drink Factors: • How many times a day do you drink: • 1. Coffee or tea with sugarbetween meals? • 2. Pop, Kool-aid, lemonade, sports drinks, fruit juice, iced tea with sugar between meals? • Total the number of these • How many glasses of water or dilute drinks do you have a day? This does not include coffee, soft drinks, full strength juice or sports drinks. • Chronic Dehydration can increase caries risk • Count 2 if the patient is dehydrated
Diet Questionnaire: • Drink Factors cont’d: • Important trend: Cariogenic drinks are on a great increase! • Huge marketing efforts have been made, and often soft drink companies have a monopoly on vending machines in schools. This has paid off with a corresponding increase in decay and acid erosion. • Consumption of soft drinks, sports drinks, fruit juices and iced tea have skyrocketed in recent years, especially among teens and adolescents. Sports drinks are meant for athletes involved in over 60 minutes of aerobic activity. Sedentary kids are drinking sports drinks after mild activity, thanks to good marketing. • Water and milk consumption is dropping.
Diet Questionnaire: Food Factors: • How many times a day do you: 1. Chew regular gum (Not sugarless)? • Eat mints, lozenges, candies or candy bars, dried fruit, energy bars between meals? • Eat sweetened baked goods (Donuts, cookies, pastries) between meals? Total the number of all of these.
Diet Questionnaire: • Do you have a habit of sipping a sweetened drink (Coffee, cola, juice) or eating a sweet snack over an extended period of time, 45 minutes or more? • If yes, add 2
Diet Questionnaire: • Total diet scores are added up, divided by 3 and this is the number used for the Caries Risk Assessment score for Diet Factors. • 0-2 Sugar exposures=0 • 3-4 Sugar exposures =1 • 5-6 Sugar Exposures =2 • >6 exposures =3
Existing Decay Previous Decay Root Caries Fluoride Exposure Diet Factors Oral Hygiene 0=Good OH 1=Fair OH PSRs <3 Mod Plaque 2=Poor OH PSRs >3 Heavy Plaque Categories for Simplified CRA
Categories for Simplified CRA • Existing Decay • Previous Decay • Root Caries • Fluoride Exposure • Diet Factors • Oral Hygiene • Additional Tests • S.mutans and Lactobacillus • Saliva Flow
Bacterial testing is done only in cases when indicated, if other results are not obvious. >1,000,000 colonies s.mutans or >100,000 lactobacillus = 2 > 4 minutes for 3cc saliva sample =2 Indicates possible Xerostomia Additional Tests S.mutans and Lactobacillus Saliva Flow Categories for Simplified CRA
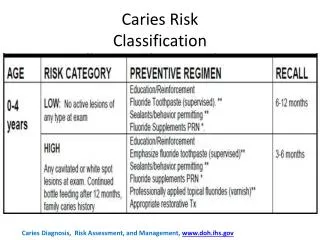
CRA Score and Caries Risk: The Total Score • 0-2 = Low Risk • 3-4 = Medium Risk • 4-6 = High Risk • >6 = Severe Risk of Caries
CRA Score and Caries Risk: Applying the data From this data we can set up custom protocols for the individual patients, including • Fluoride treatments • Frequency of X-rays • Frequency of Recall visits • Restorative decisions on borderline lesions • Whether to Observe, Seal or Restore
Application In Practice- Take-home message: • Caries Risk Assessment is an essential part of scientifically based dentistry in real general practice • A practical Caries Risk Assessment takes less than 5 minutes to do during a new patient exam, and contributes valuable data- please use my version or your own in your practice, but use it! Identify your high, medium and low risk patients. The next part of the presentation will deal with use of this data for treatment protocols.
Dr. Richard Ehrlich www.elmtreedental.com
Part 2: Diagnostic, Restorative and Preventive Protocols using Risk Analysis and High Tech instrumentation Richard Ehrlich DDS dre@elmtreedental.com
Tools needed: In addition to the usual instrumentation and radiographs for diagnosis: Diagnodent- Diagnostic Laser caries detector
Diagnodent Laser • This device can give a numerical reading of early decay in pits. • With practice, it can be more accurate than visual, tactile or radiographic examinations. • Caution is required around hypocalcifications and existing resins and sealants as the unit may misread.
Other adjuncts- Magnification • Loupes Operating Microscope Intraoral Camera
Diagnodent Laser • Readings under 10 have no decay. • Readings 10-20 usually have stain or enamel caries Readings over 35 generally have decay in dentin. Readings of 99 are decayed well into dentin. Readings 20-35 need individual assessment
Protocols using the tools • At the initial diagnosis, the patient can usually be assigned to a Risk group. • This is re-evaluated at the next recall, as often the status changes after the initial treatment.
Low Risk- Initial ProtocolCaries Index 0-2 • Observe pits and fissures with stain or early decay, decay in enamel, very early (stable) decay in dentin, old restorations, poor margins. Diagnodent (DD) < 25-30 Restore fractured restorations, obvious decay (DD>40).
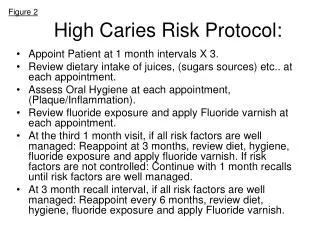
Medium Risk- Initial Protocol Caries Index 3-4 Observe stained pits, deep pits, early decay in enamel. (DD<20). Restore old restorations with cracks and broken margins, decay in pits with halo or shadow, any decay in dentin. (DD>25-30) Diet Counseling Introduction Fluoride Supplements for children in non fluoridated areas
High Risk- Initial ProtocolCaries Index >4 Observestained pits DD<10 Restore early decay in enamel and dentin. (DD>15-20) Restore old restorations with cracks and broken margins Diet Counseling Introduction Fluoride Supplements for children Prevident 5000 for Adults Fluoride varnish on incipient areas
First Re-evaluation • All patients are re-assessed after the initial treatment. • Many are at reduced risk once initial decay is removed, and diet/OH improvements are implemented.
High Risk- First Evaluation 3 month period Caries Risk Re-Evaluation, including s. mutans, lactobacillus test Salivary flow measurement • 3-month Topical Fluoride, OHI • If risk reduced, proceed to Medium Risk Recare protocol
Low Risk Suggested Protocol • Recall patient every 9 months, consider increasing if remaining low risk. • No Topical Fluoride • No Fluoride Supplement • Take BW radiographs every 3 years • OHI As needed • Observe pits and fissures with stain or early decay in enamel, very early decay in dentin. (DD<25-30) Polish or seal old restorations with poor margins, and observe Sealants not required
Medium Risk Suggested Protocol • Recall patient every 6 months • Topical Fluoride for children • Fluoride Supplement for areas without water F- • Take BW radiographs every 2 years • OHI As needed • Observe stained pits, early decay in enamelor optionally seal. (DD<15-20)
Medium Risk Suggested Protocol • Restore pits and fissures with early decay, any very early decay in dentin, old restorations with poor margins. (DD>20) Polish or seal old restorations with fair margins, and observe.
High Risk Suggested Protocol • Full diet counselling with diary
High Risk Suggested Protocol • Full diet counselling with diary • Recall patient every 3 months: • Topical Fluoride • Fluoride Varnish on susceptible areas • Take BW radiographs yearly • OHI • Home Fluoride Trays or Prevident 5000 • Chlorhexidine Rinses -Adult • Fluoride Supplements-Child • Evaluate for xerostomia
Restore pits with early decay, any very early decay in dentin or enamel, (DD>20) old restorations with fair- poor margins. Sealants/Preventve resins- all deep pits and fissures. (DD>5-20)
New Technologies: • Often high risk kids present with early decay or deep pits in barely erupted teeth. These can be very hard to seal due to access or co-operation issues. If there is any moisture contamination, traditional sealants will fail.
New Technologies: • Fluoride-releasing sealants for suspect pits with poor access • Fuji Triage can be placed quickly and easily, needing very little cooperation. Due to the fluoride release, it is less likely than traditional sealants to allow decay below if it leaks.
New Technologies: Ozone Treatment of pits A promising new technique involves sterilizing the pits and fissures with ozone. This has been shown to stop decay and even allow remineralization This may make cooperation even easier in early intervention More research is needed here.
Proposed steps in Healozone Treatment 1. Cleaning 3. Treatment 4. Reductant Fluid Promotes the immediate remineralization of the tooth. 2. Measurement
Application In Practice- Take-home message: • Identify your high, medium and low risk patients. • Treat them differently based on their risk levels. • Aim to convert all your patients to low risk, or at least reduce their caries index. • Do not over-treat your low-risk patients. They need their own preventive and restorative protocols. • Do not under-treat your high risk patients. They need every preventive and early intervention restorative measure you can give them, especially if they cannot convert to lower risk.
Summary Flow Chart- • This flow chart is available from my web page at www.elmtreedental.com
Summary • A system of numerically rating a patient’s caries risk has been presented • Protocols for minimal invasive and preventive treatment for low risk patients and maximal preventive and early restorative treatment for high risk patients have been demonstrated, to allow custom treatment for each patient.