Download
1 / 59
620 likes | 958 Views
Post Exposure Prophylaxis (PEP/oPEP). Dr Don Ajith Karawita MBBS (PERA), PgD Ven (COL), MD Venereology (COL) (Senior Registrar in Venereology) National STD/AIDS Control Programme. CDC Guidelines 2001. CDC headquarters in Atlanta. Hand washing Gloves Personal protective equipment (PPE)

E N D
Post Exposure Prophylaxis (PEP/oPEP) Dr Don Ajith Karawita MBBS (PERA), PgD Ven (COL), MD Venereology (COL) (Senior Registrar in Venereology) National STD/AIDS Control Programme
CDC Guidelines 2001. CDC headquarters in Atlanta
Hand washing Gloves Personal protective equipment (PPE) Patient care equipments Cleaning of instruments Environmental control Management of spills Linen management 7. Occupational health and blood borne pathogens Handling of sharps Prevention of mucous membrane exposures Management of needle stick accident or mucous membrane exposure Collection and transport of specimens 8. Patient isolation Standard Precautions
Additional Precautions • Transmission based precautions • Airborne precautions (droplet nuclei < 5µm) • Droplet precautions (droplet nuclei > 5µm) • Contact precautions / isolation • Strict isolation • Aseptic precautions • Cleaning of entry site of the body • Hands of the staff must be disinfected and gloved.
Alcohol Surgical spirit (60% isopropyl alcohol) 70% ethyl alcohol Alcohol hand rub (Isopropyl alcohol with glycerol) Aldehydes Cidex (2% glutaraldehyde solution) Chlorhexidines Hibisol (0.5% chlorhexidine in 70% alcohol Hibitane (4% chlorhexidine gluconate Hibiscrub (4% chlorhexidine gluconate with a detergent) Disinfectant / Antiseptic
Chlorine releasing agents TCL, Bleaching powder (Calcium hypochiorite 35% w/w of available chlorine) Sodium hypochlorite liquid form 5% stock solution 1% (10,000ppm) 0.1%(1000ppm) 0.01% (125ppm) Milton Iodophors Betadine, Wokadine (10% solution, available iodine 1%) Betadine scrub, Wokadine scrub (7.5% Povidone iodine scrub, avilable iodine 0.75% Peracetic acid Perasafe(Peracetic acid) Phenolic disinfectants Lysol(2%, 5% solutions) Disinfectant / Antiseptic
Hospital waste Hazardous waste General or Non-hazardous waste • Sharps • Infectious waste (incinaration/ Burial) • Pathologicl waste (incinaration/ Burial) • Chemical waste (Returned to supplier/ MSD) • Pharmaceutical waste (Returned to supplier/ MSD) • Radioactive waste (Keep for radioactive decay→Dispose as non hazardous waste) Dispose to common garbage site/bin Collected by local authorities
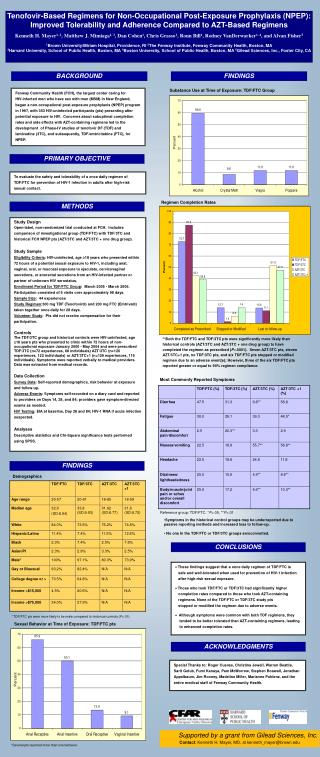
Hepatitis B Virus (HBV), Hepatitis C Virus (HCV), and Human Immunodeficiency Virus (HIV) • Bloodborne viruses • Can produce chronic infection • Transmissible in healthcare settings • Data from multiple sources (e.g., surveillance, observational studies, serosurveys) used to assess risk of occupational transmission
Risk of Bloodborne Virus Transmission after Occupational Percutaneous Exposure
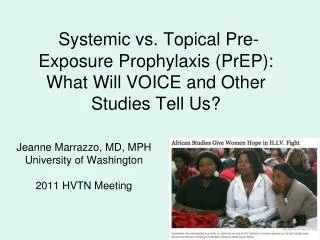
3. Determine Infectious Status of Source Patient Percutaneous Severe, Less severe Mucous membrane/Non intact skin Small volume, Large volume. 2. Exposure Substance 1.Exposure Blood, Bloody fluid, OPIM 4. Determine Susceptibility of Exposed Person Health care worker (HCW) Evaluation - Occupational exposure to infectious materials
Elements of Postexposure Management • Wound management & Exposure reporting → Step 1 • Risk Assessment → Step 2 • (1) blood borne infection status of source person • (2) Infectious material • (3) type and severity of exposure • (4) Susceptibility of HCW • Appropriate treatment → Step 3 • Follow-up, and counseling → Step 4
Step 1 Provide immediate care to the exposure site • Post exposure Wound Management: • Wash wounds and skin with soap and water • Flush mucous membranes with water • No evidence of benefit for: • application of antiseptics or disinfectants • squeezing (“milking”) puncture sites • Avoid use of bleach and other agents caustic to skin • Inform authorities → Infection control unit.
Management of sharps accidents WHO / SEAR 1999
Elements of Postexposure Management • Wound management & Exposure reporting → Step 1 • Risk Assessment → Step 2 • (1) blood borne infection status of source person • (2) Infectious material • (3) type and severity of exposure • (4) Susceptibility of HCW • Appropriate treatment → Step 3 • Follow-up, and counseling → Step 4
Infectious status of the source person (SC) presence of HBsAg presence of HCV antibody presence of HIV antibody if source unknown, assess epidemiologic and clinical evidence (Do not test discarded needles) Body substance blood bloody fluid Other potentially infectious materials (OPIM) (semen, vaginal secretions and CSF, synovial, pleural, peritoneal, pericardial and amniotic fluids) or tissue Type of exposure (EC) percutaneous mucous membrane non-intact skin bites resulting in blood exposure Determine susceptibility of exposed person (HCW) Hepatitis B vaccine status HBV immune status if vaccine response status in unknown Anti-HCV and ALT HIV antibody Postexposure Management: Risk Assessment (Seek expert advice) 1 3 4 2
Elements of Postexposure Management • Wound management & Exposure reporting → Step 1 • Risk Assessment → Step 2 • (1) blood borne infection status of source person • (2) Infectious material • (3) type and severity of exposure • (4) Susceptibility of HCW • Appropriate treatment → Step 3 • Follow-up, and counseling → Step 4
Step 3 Give PEP for exposures posing risk of infection transmission • HBV • Give oPEP as soon as possible within 24 hours. • PEP can be given to pregnant women • HCV • PEP not recommended • HIV • Initiate PEP within hours of exposure (2-72 Hours) • Offer pregnancy testing to all women of child bearing age not known to be pregnant. • Seek expert consultation if viral resistance suspected. • Administer PEP for 4 weeks if tolerated.
Concentration of HBV in Body Fluids HighModerate Low/Not Detectable BloodSemen Urine SerumVaginal FluidFeces Wound exudatesSaliva Sweat Tears Breast Milk
Persons who have previously been infected with HBV are immune to reinfection and do not require PEP. • Hepatitis B immunoglobulin: dose 0.06ml/kg im • A responder is a person with adequate levels of serum antibody to HBsAg (i.e. anti-HBs > 10mIU/ml): a non-responder is a person with inadequate response to vaccination (i.e. serum anti-HBs antibody< 10mIU/ml) • The option of giving one dose of HBIG and reinitiating the vaccine series is preferred for non-responders who have not completed a second 3-dose vaccine series. For those who previously completed a second vaccine series but failed to respond, 2doses of HBIG are preferred. Give one dose at time of exposure, and the second dose one month later.
Hepatitis B Vaccine: Long-Term Efficacy • Anti-HBs titers decline to <10 mIU/mL in 30-50% of adults within 8-10 years after vaccination • Exposure to HBV results in anamnestic anti-HBs response that prevents clinically significant HBV infection • Immune memory remains intact for at least 20 years after immunization • Chronic HBV infection rarely documented among vaccine responders • Booster doses currently not recommended
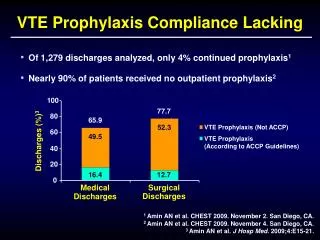
Overview of the HIV clinical disease AIDS Clinical stage 4 AIDS Defining illnesses HIV Seroconversion illness Clinical stage 3 Clinical stage 2 75% 33% Clinical stage 1 3wks 1-4wks 8 to 12 years
If drug resistance is a concern, obtain expert consultation. Initiation of PEP should not be delayed pending expert consultation and, because expert consultation alone cannot substitute for face-to-face counseling, resource should be available to provide immediate evaluation and follow-up care for all exposures. • The designation “consider PEP” indicates that PEP is optional and should be based on as individualized decision between the exposed person and the treating clinician. However, consider basic 2-drug PEP for a source with HIV risk factors, or occurs in a setting where exposure to HIV-infected persons is likely. • If PEP is offered and taken, and the source is later determined to be HIV negative, PEP should be discontinued. • For skin exposures, follow-up is indicated only if there is evidence of compromised skin integrity (e.g. dermatitis, abrasion, or open wound)
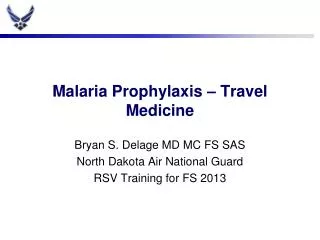
Considerations When Using PEP Risk of Transmission Risk of Adverse Effects PEP