Download
1 / 14
140 likes | 212 Views
Maryland How Do Premiums Affect Enrollment?. Tricia Roddy Maryland Department of Health and Mental Hygiene June 28, 2004. Maryland’s HealthChoice Program Provides Services To 75% Of All Medicaid Recipients. Managed Care Program – HealthChoice. Based on January 2004 enrollment.

E N D
MarylandHow Do Premiums Affect Enrollment? Tricia Roddy Maryland Department of Health and Mental Hygiene June 28, 2004
Maryland’s HealthChoice Program Provides Services To 75% Of All Medicaid Recipients Managed Care Program – HealthChoice Based on January 2004 enrollment
Budgetary Language Expanded Premium Requirements To More Recipients Prior to FY 2004 • The income standard for MCHP Premium was between 200% and 300% of FPL • Premiums are set at 2% of the annual income of a family of two, regardless of the actual number of children • $41 for incomes between 200% and 250% of FPL • $52 for incomes between 250% and 300% of FPL FY 2004 - General Assembly Budgetary Language • The income standard for MCHP Premium was expanded to include children with family income of 185% to 200% of FPL for FY 2004 only • Premiums were set at 2% of the annual income of a family of two at 185% of FPL, regardless of the actual number of children ($37 per family per month)
The Number Who Disenrolled Was Lower Than Expected • An Urban Institute study estimated declines in enrollment of 16% when participants are charged premiums that equal 1% of family income, enrollment declines of about 49% if premiums equal three percent • In Maryland, the decline in enrollment (28%) was lower than expected for this population group Source: Leighton Ku. “Charging The Poor More For Health Care: Cost-Sharing in Medicaid.” Center on Budget and Policy Priorities. May 7, 2003.
Premium’s Impact On Enrollment Was Immediate and Somewhat Temporary • Since December 2003, enrollment has been steadily growing • Between November 2003 and January 2004, enrollment grew by 10% • In a comparable period last year, enrollment was relatively static • As of March 31, 2004, 158 (or 9%) disenrollees have re-enrolled
Department Conducted Survey To Study The Premium Expansion • Determine the impact of the premium on enrollment • Determine whether families had obtained other health coverage since their children disenrolled • Determine whether there were differences between enrollees and disenrollees in terms of utilization, family size, age, race/ethnicity, and geography
Premium Not The Main Reason For Why Children Disenrolled • 360 parents/guardians were surveyed in February 2004 • Key Findings • A majority said the premium was not the main reason their child left MCHP • 63% thought $37/month per family was affordable • Over half said they had obtained other health insurance for their child
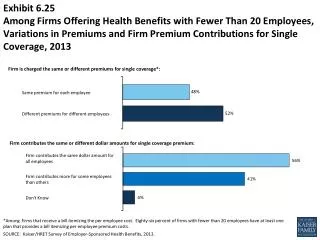
While Enrolled, Children Who Disenrolled Were Less Likely to Access Services Percentage of the Population Accessing Well-Child Services by Age, CY 2002 Source: Maryland encounter data
Families With More Than One Child Were More Likely To Stay On The Program Distribution of Family Size for Children in 185-200% FPL Families • Families with 1 child accounted for the majority of disenrollment between Sept. 03 and Jan. 04
A Slightly Larger Proportion Of African-Americans Disenrolled Racial/Ethnic Distribution of Children who Disenrolled Compared to Children who Remained Enrolled (12/31/03) Source: Maryland encounter data
Very Little Difference With Regard To Age Distribution Age Distribution of Children who Disenrolled Compared to Children Who Remained Enrolled(12/31/03) Source: Maryland encounter data
Little Differences Among Geographic Regions Regional Distribution of Children Who Disenrolled Compared to Children who Remained Enrolled(12/31/03) Source: Maryland encounter data
Lessons Learned • Survey findings indicate that the premium did not cause the majority of disenrollments • Most of the disenrolled had obtained other insurance • Disenrolled children used fewer services while enrolled • Disenrolled children were more likely to be in families with only one child enrolled • There were few differences between enrolled and disenrolled children with regard to age, race/ethnicity, or region
What Does This Mean For Maryland? • Cost sharing should be explored before making more serious cuts, such as reductions in services and eligibility • CMS should reevaluate its cost sharing policies • Cost sharing should be explored when designing new programs to cover more of the uninsured