Download
1 / 30
300 likes | 457 Views
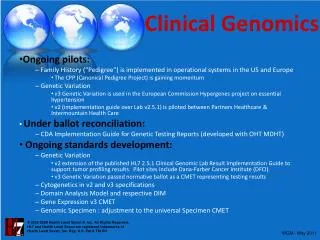
Establishing a Clinical Genomics Program at an Academic Medical Center. Jason Merker, M.D., Ph.D. Co-director, Stanford Clinical Genomics Service Regional APC/PDAS Meeting, Kauai 10/23/2014. Introduction to Clinical Genomics ( in 5 Slides). Wellcome Collection – Medicine Now.

E N D
Establishing a Clinical Genomics Program at an Academic Medical Center Jason Merker, M.D., Ph.D. Co-director, Stanford Clinical Genomics Service Regional APC/PDAS Meeting, Kauai 10/23/2014
Introduction to Clinical Genomics (in 5 Slides)
Wellcome Collection – Medicine Now • 3.4 billion units of DNA code: • 127 volumes • 1,000 pages per volume
Some mutation types are difficult to detect by genome or exome sequencing technologies
Introduction to Clinical Genomics at Stanford
Clinical Genomics Efforts at Stanford Basic, Translational, and Clinical Research Clinical Genomics Service GenePool Biobank
Stanford Clinical Genomics Service • Directors– Jason Merker (Path), Euan Ashley (CV Med) • Department – Pathology • Goal– Build a clinical laboratory service at Stanford University Medical Center that uses genome sequencing to evaluate adult and pediatric patients with unexplained genetic diseases. • Pilot – Develop analysis/curation pipeline and perform genome sequencing on 4 patient populations (100 cases total): • Heritable cancer predisposition • Heritable cardiovascular disorders • Pediatric syndromes • Familial adverse drug reactions or sensitivity
Workflow – 1 Test RequestPatient and physician request genome sequencing for heritable disease through EMR • Review by Genetic • Test Consultation Service • Genetic Counselor • Molecular Pathologist • Medical Geneticist • Establish questions being posed by • patient and treating team • Genetic? • Candidate variants and analysisapproach • Clinical use
Workflow – 2 • Patient meets with genetic • counselor • Clinical counseling & consent • *Options for return of secondaryfindings • 2-step consent process for non-actionable findings • Biobanking and data-sharing counseling & consent Insurance authorization • Blood draw • 1 tube for genome sequencing • 1 tube for confirmatory studiesand specimen ID • 1 tube for biobanking (with appropriate consent)
Workflow – 3 Illumina genome sequencing • Variant filtering/prioritization • Phenotype • Inheritance pattern • Predicted deleterious • Secondary findings • Data analysis (open source, commercial, and Stanford developed): • Alignment • Variant calling • Quality management • ID and gender checks to confirm specimen identity
Workflow – 4 • Genomics Review Groups • Genomics Service • Treating Team • Content expert • Variant verification by orthogonal method • Segregation analysis Curation meeting and draft report
Workflow – 5 Final report generated and uploaded to EMR Patient meets with genetic counselor and relevant members of treatment team • Yearly re-analysis upon request • Improved analysis • Improved sequencing • Increased medical knowledge
Case 1 – 30 YOM w/ DCM • TTN A-band truncating variant that segregates with disease in large family – likely pathogenic • RYR1 variant (malignant hyperthermia) – likely pathogenic vs. variant of uncertain significance
Clinical Genetic Test Consultation ServiceRationale #1 – The number of clinical genetic tests is becoming unmanageable The CDC estimates that genetic tests for use in the clinical setting have been developed for approximately 2,000 diseases
Clinical Genetic Test Consultation ServiceRationale #2 – The number of misorders for complex genetic testing is high “Approximately 25% of all requests for complex genetic tests assessing germ line mutations were changed following review.” Miller CE et al. 2014. Am J Med Genet Part A 164A:1094–1101.
Clinical Genetic Test Consultation Service – Summary of rationales • The number, indications, and complexity of genetic tests offered have been increasing, and will continue to do so for the foreseeable future. • It is therefore not surprising that mistakes often occur in the ordering of complex genetic tests. • Incorrect ordering of genetic tests results in unnecessary costs to the healthcare system, but more importantly adversely affects the care of our patients • Failure or delays in getting the needed test results • Communication of results from the incorrect test • Providing genetic information that was neither requested nor desired by the patient
Clinical Genetic Test Consultation Service – Personnel Molecular Pathologist Genetic Counselor Medical Geneticist
Clinical Genetic Test Consultation Service • Provide consultation to SUMC healthcare providers needing further information on available genetic testing. • Review all quests for send-out genetic testing from Stanford Clinical Laboratories to identify and help correct genetic test misorders. • Work with Genetic Test Utilization Committee develop innovative, provider-friendly ways to educate our physicians about genetic test utilization (e.g., pop-up windows in EMR offering test consultation or other educational information). • Assist departments and divisions with educational activities related to genetic test utilization (e.g., seminars, presentation to new residents) and with establishing protocols for genetic test ordering for common use cases
Open Didactic Core Curriculum in Genomic Medicine • Experimental methods for measuring and manipulating DNA/RNA • Fundamentals of human genetic variation • Microarrays and analysis of hybridization data • Sequencing methods • Heritable genetic disorders • Acquired mutations in human cancers I: solid tumors • Acquired mutations in human cancers II: hematopoietic malignancies • Pharmacogenomics • HLA genetics • Ethical, legal, and economic implications of clinical genomic testing Schrijver I et al. J Mol Diagn. 2013;15:141.
Elective Course in Advanced Genomic Medicine • Next-generation sequencing methods 2.0 • Human genetic variation 2.0 • DNA sequence analysis methods I: sequence databases andfiles • DNA sequence analysis methods II: sequence alignmentalgorithms • DNA sequence analysis methods III: genome assembly andanalysis • Introduction to scripting programming languages • Statistical tools for sequence analysis and genomics Schrijver I et al. J Mol Diagn. 2013;15:141.
Elective Course in Advanced Genomic Medicine • Next-generation sequencing methods 2.0 • Human genetic variation 2.0 • DNA sequence analysis methods I: sequence databases andfiles • DNA sequence analysis methods II: sequence alignmentalgorithms • DNA sequence analysis methods III: genome assembly andanalysis • Introduction to scripting programming languages • Statistical tools for sequence analysis and genomics Schrijver I et al. J Mol Diagn. 2013;15:141.
New Elective Course in Advanced Genomic Medicine • Genome and exome analysis for heritable disease • Tumor/normal sequencing analysis • RNA sequencing analysis • Unix commands and basic scripting