Download
1 / 22
220 likes | 356 Views
Is Bivalirudin Monotherapy Sufficient for Diabetic Patients with Acute Coronary Syndrome Undergoing PCI?. Frederick Feit, Steven Manoukian, Ramin Ebrahimi, Charles Pollack, Magnus Ohman, Michael Attubato and Gregg Stone. Is Bivalirudin Monotherapy Sufficient for Diabetic Patients

E N D
Is Bivalirudin Monotherapy Sufficient for Diabetic Patients with Acute Coronary Syndrome Undergoing PCI? Frederick Feit, Steven Manoukian, Ramin Ebrahimi, Charles Pollack, Magnus Ohman, Michael Attubato and Gregg Stone
Is Bivalirudin Monotherapy Sufficient for Diabetic Patients with Acute Coronary Syndrome Undergoing PCI? Conflicts: Shareholder: Johnson and Johnson, Medicines Co., Millenium Pharmaceuticals; Consultant: Medicines Co.
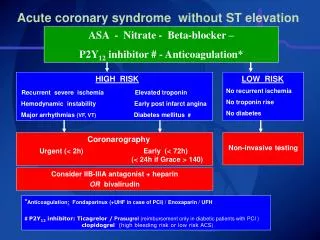
PCI for ACS in Diabetics: Metabolic Abnormalities • Increased blood glucose causes coronary artery inflammation and is prothrombotic • Increased generation of thrombin, CRP, fibrinogen, von Willebrand factor, factors VII and VIII, and platelet factor 4 • Increased expression of platelet activation markers including p-selectin, which mediates platelet-leukocyte interactions • Higher proportion of platelets expressing GPIIb/IIIa receptors
PCI for ACS in Diabetics: Background • Based on prior data including a meta-analysis of ACS trials current clinical guidelines recommend the use of GPIIb/IIIa inhibitors (GPI) in diabetic patients with ACS, especially those in whom PCI is planned1 • In the ACUITY Trial 13,819 pts, including 3852 diabetics, with moderate or high risk ACS, undergoing an early invasive strategy were randomly assigned to either the standard of care: Heparin (UFH or enoxaparin) + GPI; or, Bivalirudin + GPI; or Bivalirudin with provisional GPI 1. Roffi et al. Circulation.2001;104:2767-71
PCI for ACS in Diabetics: Methods • We compared adverse events: composite ischemia (death, nonfatal MI, unplanned ischemia driven revascularization), major bleeding and net clinical outcome (composite ischemia or bleeding) within the first 30 days in diabetic vs. nondiabetic pts • We compared the same 30-day end points in diabetic pts by treatment group
ACS: Unstable angina or NSTEMI, N=13,819 Chest pain >10’ within 24 hours, plus Biomarker +, or Dynamic ECG changes, or Documented CAD or all other TIMI risk criteria ASA Clopidogrel per local practice Bivalirudin + IIb/IIIa inhibitor Enoxaparin or UFH + IIb/IIIa inhibitor Bivalirudin + IIb/IIIai Cath within 72 hours PCI, CABG or medical management 30 day endpoints Death, MI, IUR, ACUITY major bleeding (net clinical outcome) ACUITY Design Prior UFH, LMWH (1 dose), eptifibatide and tirofiban were allowed Stone et al. Presented 2006; ACC
Study Medications • Anti-thrombin agents (started pre angiography) 1 Target aPTT 50-75 seconds 2 If last enoxaparin dose ≥8h - <16h before PCI; 3 If maintenance dose discontinued or ≥16h from last dose 4 Discontinued at end of PCI with option to continue at 0.25mg/kg for 4-12h if IIb/IIIa inhibitor not used 5 Bivalirudin option for off-pump same as PCI dose. For on-pump bivalirudin discontinued 2 hours before 6 Option to continue with pre-PCI anti-thrombotic regimen at physician discretion
PCI for ACS in Diabetics: Angiographic Triage * - p<0.001
PCI for ACS in Diabetics: Baseline Characteristics * CrCL <60 mL/min
PCI for ACS in Diabetics: 30-Day Outcomes Diabetes vs. No Diabetes P = 0.008 P = 0.15 P < 0.001 †Heparin=unfractionated or enoxaparin
Diabetic ACS Patients Undergoing PCIBaseline Characteristics by Treatment Group * creatinine clearance <60 mL/min †Heparin = unfractionated or enoxaparin
Diabetic ACS Patients Undergoing PCI: Baseline High Risk Features by Treatment Group †Heparin = unfractionated or enoxaparin
Diabetic ACS Patients Undergoing PCI: Intervention Type †Heparin = unfractionated or enoxaparin All comparisons p= NS
Diabetic ACS Patients Undergoing PCI: GP IIb/IIIa Inhibitor Administration
P = 0.27 P = 0.48 P = 0.51 Diabetic ACS Patients Undergoing PCI: 30-Day Endpoints by Treatment Group Heparin* + GP IIb/IIIa vs. Bivalirudin + GP IIb/IIIa *Heparin = unfractionated or enoxaparin
P = 0.08 P = 0.42 P = 0.003 Diabetic ACS Patients Undergoing PCI: 30-Day Endpoints Heparin* + GP IIb/IIIa vs. Bivalirudin alone *Heparin = unfractionated or enoxaparin
PSup = 0.42 PSup = 0.26 PSup = 0.57 PSup = 0.74 Diabetic ACS Patients Undergoing PCI: Components of Ischemic Endpoint Heparin* + IIb/IIIa vs. Bivalirudin Alone *Heparin=unfractionated or enoxaparin
Diabetic ACS Patients Undergoing PCI: Myocardial Infarction Classification* Heparin† + IIb/IIIa vs. Bivalirudin Alone p = 0.57 6.3% 5.6% 30 day events (%) Q-wave 1.7% p = 0.08 Q-wave 0.7% Non Q-wave Non Q-wave p = 0.79 4.9% 4.6% Heparin + IIb/IIIa Bivalirudin alone (N=703) (N=721) *CEC-adjudicated †Heparin=unfractionated or enoxaparin
Diabetic ACS Patients Undergoing PCI: Bleeding Endpoints 30-days *P value for bivalirudin alone vs. heparin + IIb/IIIa inhibitor †Heparin=unfractionated or enoxaparin
Insulin-dependent Diabetic ACS Patients Undergoing PCI: 30-Day Endpoints by Treatment Group Heparin† + GP IIb/IIIa vs. Bivalirudin alone P = 0.08 P = 0.42 P = 0.04 †Heparin=unfractionated or enoxaparin
Diabetic Patients with ACS Undergoing PCI: Conclusions • Compared with non-diabetics, diabetic patients have worse net clinical outcomes at 30 days (14.9% vs. 12.6%; p=0.008), resulting from similar rates of the composite ischemic end point (9.5% vs. 8.5%; p=0.15) and a significantly higher rate of major bleeding (7.5% vs. 5.3%; p=0.008) • In diabetic patients, compared with the standard of care, heparin (UFH or enoxaparin) + GPIIb/IIIa, bivalirudin + GPIIb/IIIa was not better for protection from ischemic events or bleeding and resulted in similar net clinical outcome
Diabetic Patients with ACS Undergoing PCI: Conclusions • Compared to those receiving the reference standard, diabetics receiving bivalirudin monotherapy, with provisional GPIIb/IIIa in 7.9%, had similar protection from ischemic events (8.3% vs. 9.5%; p=0.42) and a marked reduction in major bleeding (4.6% vs. 8.5%; p=0.003) with a trend towards improved net clinical outcome (12.1% vs. 15.2%; p=0.08) • These 30-day outcomes suggest that bivalirudin monotherapy is safe and effective for diabetic patients with ACS undergoing PCI, including those requiring insulin • One-year clinical and economic data will determine whether this regimen will become the standard of care for these patients.