Download
1 / 72
720 likes | 827 Views
This presentation will probably involve audience discussion, which will create action items. Use PowerPoint to keep track of these action items during your presentation In Slide Show, click on the right mouse button Select “Meeting Minder†Select the “Action Items†tab

E N D
This presentation will probably involve audience discussion, which will create action items. Use PowerPoint to keep track of these action items during your presentation • In Slide Show, click on the right mouse button • Select “Meeting Minder” • Select the “Action Items” tab • Type in action items as they come up • Click OK to dismiss this box • This will automatically create an Action Item slide at the end of your presentation with your points entered. Annual MeetingofAssociation of State and Territorial Public Health Nutrition DirectorsJune, 2007 Peter C. van Dyck, MD, MPH Associate Administrator for Maternal and Child Health
MCHB BUDGET 2008
MCH Formula and Allocation • Whenever the total appropriation exceeds $600 million; • 12.75% of the amount is used to fund the Community Integrated Service System (CISS) set-aside program • Remainder is allocated as 85% to States and 15% retained by the Secretary for SPRANS projects
MCH Budget for 2005, 2006, 2007, and 2008(PB)(millions) FY2005 2006 2007 2008(PB) • MCHBG…723.9....$692.5….$693.0….$693.0 • State….…$591.0....$566.1…..$566.5.…..$578.9 • SPRANS..$102.7......$99.9…....$99.9……$102.2 • CISS….…..$14.6…….$10.6…...$10.6………$11.9 • Earmark...$15.5…….$15.9….…$16.0………------ 1-numbers may not add due to rounding
MCH Budget for 2005, 2006, 2007, and 2008(PB)(millions) FY2005 2006 2007 2008(PB) • Healthy Start$102.5…$101.4…$101.5.$100.5 • Hearing………...$9.8 ..…$9.8…….$9.8…..----- • EMSC…………..$19.8….$19.8…..$19.8…..----- • TBI……………..…$9.3..…$8.9…...$8.9…...----- • Sickle Cell……...$0.2……$2.2…...$2.2……$2.2 • Family to Family.$.0…...$0.0…...$3.0…..$4.0 1-numbers may not add due to rounding
MCH Budget for 2005, 2006, 2007, and 2008(PB)(millions) 2005 2006 2007 2008(PB) SPRANS Earmarks • Oral Health…..$4.96…...$4.80……$4.80……$0.0 • Sickle Cell….…$3.97…...$3.84……$3.84……$0.0 • Epilepsy……....$2.98…...$2.88……$2.88……$0.0 • Genetics….……$1.98…...$1.92..…$1.92……$0.0 • Mental Health.$1.59…...$1.54…...$1.54……$0.0 • Fetal Alcohol…..----……..$0.99…..$0.99….…$0.0 1-numbers may not add due to rounding
Numbers Served In MCH Block Grant Program, 1997 And 2005 SOURCE: TITLE V INFORMATION SYSTEM
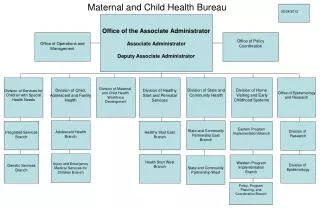
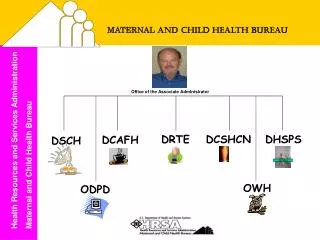
MCH Bureau DATA
Most Common Needs Identified in 2005: Preliminary Findings Healthy Lifestyles • 44 States in 2005 vs 21 in 2000 • Healthy lifestyles - general • Reduce obesity and overweight 25 States vs 10 States • Promote nutrition and/or exercise 17 States vs 7 States
18 National Performance Measures • 11) The percent of mothers who breastfeed their infants at 6 months of age. (Revised in 2006 from “The percent of mothers who breastfeed their infants at hospital discharge.”) • 14) Percentage of children, ages 2 to 5 years, receiving WIC services with a Body Mass Index (BMI) at or above the 85th percentile. (New performance measure beginning in 2006.)
The 37 Discretionary Performance Measures • 08) Percent of graduates of MCHB long-term training programs that demonstrate field leadership after graduation • 33) The degree to which a State system for nutrition services has been established for MCH populations
State Performance Measures Keyword Search • Nutrition/Physical Activity • 50 States with 84 Performance Measures • In 2000, 41 States with 60 Performance Measures • Obesity • 39 States with 48 Performance Measures • In 2000, a total of 20 State Performance Measures related to overweight/obesity in children and adolescents (no keyword search for obesity).
The National Survey of Children’s Health (NSCH) Survey Questions: • Height and Weight • Food allergy or digestive problem • Breast feeding (0-5) • How concerned are you about eating disorders (6-17)
The National Survey of Children’s Health • The 2003 NSCH was conducted by the Maternal and Child Health Bureau and the National Center for Health Statistics using the State and Local Area Integrated Telephone System mechanism (SLAITS) • Its purpose was to produce national and state-based estimates on the health and well-being of children, their families, and their communities
The Children’s Health Survey AK AK HI HI
Breastfeeding Legislation in the U.S.by State (from www.lalecheleague.org)
Highlights from the National Survey of Children’s Health • Overall, 84.1 percent of children are reported to be reported to be in excellent or very good health. • The NSCH found that 14.8 percent of 10- to 17-year olds are considered overweight using parent-reported height and weight. • Males are more likely than females to be overweight. • Levels of physical activity and sports participation appear to be linked to overweight in children. Parental exercise also appears to be related.
Highlights from the National Children’s Health Survey • As family income rises, overweight falls. • The occurrence of overweight declines with age (21.9 percent of 10- to 11-year olds compared to 10.7 percent of 15- to 17-year olds. • Rural children are more likely to exercise regularly than children in urban areas. • Children in both large and small rural areas are significantly less likely to be breastfed for at least 6 months.
MCH Bureau NUTRITION STRATEGIC PLAN
Nutrition Strategic Plan • Framework for cross-division collaboration and coordination in developing and implementing nutrition and breastfeeding activities in MCHB. • 5-year plan (FY 2002-2006) • Plan to be updated for FY 2007-2011
MCHB Cross-Division Nutrition Committee • MCHB Nutrition Strategic Plan focuses on four major areas: • Breastfeeding Promotion and Support • Overweight/Obesity Prevention and Healthy Lifestyle Promotion • Public Health Nutrition Leadership and Training • Coordination and Collaboration with Federal, State and Local Partners
MCHB Cross-Division Nutrition Committee • MCHB Nutrition Strategic Plan focuses on four major areas: • Breastfeeding Promotion and Support
Breastfeeding Support • Systems Support • Liaison to the U.S. Breastfeeding Committee • Strategic Plan for Breastfeeding in the U.S. • National Breastfeeding Coalition Workshop (2008) • Provider Support • Academy of Breastfeeding Medicine • Development of protocols and support for annual meeting.
Breastfeeding Provider Support • AAP Breastfeeding Promotion in Physicians’ Office Practices (BPPOP) – Project Ending Summer 2007 • Focused on educating and supporting future and practicing physicians and health care professionals in culturally effective breastfeeding promotion and support – directed at achievement of Healthy People 2010 goals. • Developed breastfeeding curriculum for medical residency training programs, which has been tested and is currently undergoing evaluation. • http://www.aap.org/advocacy/bf/bppopIII.htm
Breastfeeding Support • Worksite Support • New HRSA resource kit developed to improve lactation support in the workplace. • Goals are to 1) increase awareness among employers of the economic benefits of breastfeeding; 2) outline manageable and flexible models for implementing or enhancing a worksite breastfeeding support program, and 3) increase the number of U.S. employers that utilize a worksite breastfeeding support program.
Breastfeeding Worksite Support (in process) • Resource Kit for: • Employers • Human Resource Managers • Lactation Consultants • Employees DRAFT
Proposed Resource Kit Components • An outreach & marketing guide for advocates. • Return on investment & other key considerations foremployers. • General steps to building a lactation support program for workplace managers. • Template documents. • An employees’ guide to breastfeeding & working.
MCHB Cross-Division Nutrition Committee • MCHB Nutrition Strategic Plan focuses on four major areas: • Breastfeeding Promotion and Support • Overweight/Obesity Prevention and Healthy Lifestyle Promotion
Overweight and Obesity • May 2006 workshop convened by NRC and IOM, NAS • Report (released in February 2007) summarizes research discussed and reviews U.S. trends in maternal weight prior to, during and after pregnancy among different populations of women.
Influence of Pregnancy Weight on MCH • Workshop presentations indicated that almost 30 percent of women of childbearing age are obese, and the prevalence of obesity is higher among Mexican American and non-Hispanic black women. • Over 15 percent of adolescent girls are overweight, with higher prevalence rates among non-Hispanic black adolescents. • Based on limited data from 1983-2004, prepregnancy underweight declined, while the prevalence of prepregnancy overweight increased. • Only about one-third of women gain within the 1990 IOM-specified ranges during their pregnancies.
Influence of Pregnancy Weight on MCH • Past efforts to advise women on weight for pregnancy (before, during and after) focused primarily on insufficient gestational weight gains and concerns about low birth weight. • Data are limited on the individual, psychosocial, community-based , and health care and health care system factors that may help women comply with recommended weight and gestational weight guidelines during and after pregnancy. • Key social predictors of gestational weight gain include smoking, SES, education, use of illegal substances, diet, physical activity, unintended pregnancy, domestic violence, eating disorders, and provider advice.
Influence of Pregnancy Weight on MCH Key Messages: • Absence of Adequate Data Systems - no national surveillance system exists to adequately monitor maternal weight prior to, during and after pregnancy. There is a need for improved data collection systems to monitor maternal weight and weight gain during pregnancy. When race/ethnicity is considered in the literature, major groups (e.g., Asian, American Indian and Hispanic groups) are underrepresented.
Influence of Pregnancy Weight on MCH Key Messages (continued) • Recognize Research Advances as well as Gaps – Differentiate among diverse components of gestational weight gain and patterns and timing of weight gain. New data on predictors of gestational weight gain remain limited in scope. There is a need to consider important sub-groups (e.g., racial/ethnic groups, women who are obese prior to pregnancy, and adolescents.)
Influence of Pregnancy Weight on MCH Key Messages (continued) • Achieve and Maintain Appropriate Weight Gain Few studies can be found in the literature that describe interventions for achieving appropriate weight before, during and after pregnancy. The impacts of pre-pregnancy and post-partum weight patterns on maternal and child health outcomes need to be explored.
Influence of Pregnancy Weight on MCH Key Messages (continued) • Update 1990 Recommendations – most commonly expressed view at the workshop was that the 1990 recommendations need to be updated, specifically for obese women and adolescents. Any effort to update the recommendations should strive to link new recommendations directly to specific, and more diverse, pregnancy outcomes. The changing demographics (age, race and ethnicity) of the childbearing population also need to be recognized.
Child and Adolescent Overweight and Obesity • Expert Panel Convened in February 2005 to Develop Recommendations for the Prevention, Assessment, and Treatment of Child and Adolescent Overweight/Obesity (AMA in collaboration with HRSA and CDC) • Committees’ recommendations will be released in Pediatrics Journal supplement in 2007.
National Business Group on Health • MCHB nutrition staff serve on the Obesity Institute, an initiative that encourages members to: • Network with other corporate leaders to raise awareness about the health and cost consequences of obesity. • Identify and test solutions to obesity that have a positive return on investment. • Advance health plans’ and vendors’ efforts to implement solutions.
National Business Group on Health • With MCHB support, developed An Employer Toolkit for Addressing Overweight Among Employees and Their Children. • Toolkit includes: • Issue Brief • PowerPoint Presentation • Family Fact Sheets • Tip Sheets
Overweight and Obesity • MCHB Nutrition Strategic Plan supports the funding of interdisciplinary training for health providers working as a team to: 1) treat pediatric overweight/obesity 2) develop intervention/prevention programs. (motivational interviewing techniques) (Funding support provided to the University of Alabama at Birmingham and University of Minnesota.)
Innovative Approaches To Promoting a Healthy Weight in Women • Purpose: to develop creative, innovative approaches that are effective in reducing the prevalence of overweight/obesity in women. • Efforts must target women in communities with limited access to preventive health services, particularly women of color, who are disproportionately affected by this risk factor.
Innovative Approaches to Promoting a Healthy Weight in Women • Approaches must be substantive in nature and incorporate nutrition, physical activity and health/wellness components. • Must also link women, when appropriate, with Title V/other relevant services to provide comprehensive care.
Innovative Approaches to Promoting a Healthy Weight in Women • 12 Grantees have been funded, beginning in September 2004 for approximately $150,000/year for 3 years • Texas State University, San Marcos, TX • NorthEast Ohio Neighborhood Health Services (NEON), Cleveland, OH • Holyoke Health Center, Holyoke, MA
Funded May 2005 Mariposa Community Health Center, Nogales, AZ Orange County Health Department, Orlando, FL Bad River Band of Lake Superior Chippewa Indians, Odanah, WI Christiana Care Health Services, Inc., Wilmington, DE Funded August 2006 Southeast Alaska Regional Health Consortium, Sitka, AK White Mountain Apache Tribe, Whiteriver, AZ University of Michigan, School of Social Work, Ann Arbor, MI Spectrum Health Hospitals, Grand Rapids, MI Erie Family Health Center, Inc., Chicago, IL Innovative Approaches To Promoting a Healthy Weight in Women