Download
1 / 45
460 likes | 689 Views
Drotrecogin alfa (activated). Randy Wax, MD, FRCP(C) Staff Intensivist and Education Director Mount Sinai Hospital Department of Medicine University of Toronto. Objectives. Understand trial design of PROWESS Evaluate the impact of the single protocol amendment during the trial

E N D
Drotrecogin alfa (activated) Randy Wax, MD, FRCP(C) Staff Intensivist and Education Director Mount Sinai Hospital Department of Medicine University of Toronto
Objectives • Understand trial design of PROWESS • Evaluate the impact of the single protocol amendment during the trial • Evaluate the overall benefit of activated Protein C for severe sepsis • Consider the results of sub-group analyses • Safety profile during PROWESS • Some real case examples
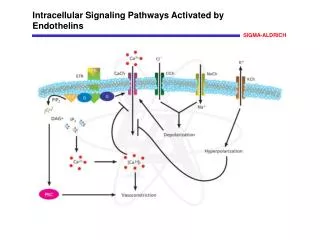
Organ failure A new understanding of sepsis pathophysiology Sepsis Coagulation Fibrinolysis Endothelial injury Inflammation Death
Study design • Randomized, double-blind, placebo-controlled study in adult patients with severe sepsis • 164 sites in 11 countries • Planned 2280 patients • Single-dose study • 24 mg/kg/hrdrotrecogin alfa (activated) infusion or placebo for 96 hours 6510.01
Study design • Primary objective • Effect on 28-day all-cause mortality • Secondary objectives • Safety • Effect on organ function • Pharmacokinetics and pharmacodynamics
Study Design 28-day all-cause mortality assessed Start of study drug infusion 24 hr to meet entry criteria Routine Patient Care 24 hr from meeting entry criteria to start of drug End of 96-hour infusion of study drug W. Macias, Eli Lilly
Study design • Inclusion criteria = Severe Sepsis • Known or suspected infection • Evidence of a systemic response to infection • Three or four of the criteria defining SIRS • One or more sepsis-induced organ dysfunctions • Cardiovascular • Respiratory • Renal • Hematologic • Metabolic acidosis
Study design • Exclusion criteria • High risk of bleeding - similar risk assessment as for systemic heparin • Systemic heparin and anti-platelet agents (except ASA) • Platelet count <30,000/mm3 • End stage liver disease • End stage renal disease (on RRT)
Study design • Exclusion criteria • HIV with CD4 count <=50/mm3 • Bone marrow, lung, liver, pancreas, or small bowel transplantation • Organ failure >24 hours in duration at time all entry criteria met
Study design • Exclusion criteria • Moribund and where death is imminent • Not expected to survive 28 days due to underlying non-sepsis related condition • Patient advance directive to withhold life-support with the exception of CPR • Family not committed to aggressive management of patient • Primary physician not committed to aggressive management of patient
Prowess Study: Amendment Minor Changes to Inclusion Criteria • Original protocol: Allowed respiratory organ failure (PaO2/FiO2) to be calculated by % saturation • Amended protocol: Required respiratory organ failure (PaO2/FiO2) to be calculated by blood gas • Original protocol: Allowed metabolic organ failure to be either low pH or elevated lactic acid concentration • Amended protocol: Required metabolic organ failure to be both low pH and elevated lactic acid concentration W. Macias, Eli Lilly
Prowess Study: Changes to Exclusion Criteria with Amended Protocol • Original protocol: "Patients with high probability of dying from underlying non-sepsis condition within the 28-day study period were excluded." • Amended protocol: clarified the following exclusion criteria: • "Known or suspected portal hypertension" changed to include clinical manifestations – esophageal varices, chronic jaundice, cirrhosis, or chronic ascites • "Not expected to survive 28 days given preexisting medical condition" changed to "… preexisting uncorrectable medical condition." Examples were provided. Enrollment of patients with malignancy must have had prior approval by coordinating center W. Macias, Eli Lilly
Prowess Study: Changes to Exclusion Criteria with Amended Protocol • The following populations were excluded: • Patients with bone marrow, lung, liver, pancreas, or small bowel transplantation • Patients who were moribund and death was imminent • Patients whose family had not committed to aggressive management of patient • Patients whose 1st organ failure >24 hours in duration at time of meeting all inclusion and exclusion criteria W. Macias, Eli Lilly
Date Event 7/28/1998 First patient enrolled 3/ 0 5/1999 Protocol amendment approved by Lilly 6/ 0 6/1999 First patient enrolled under amendment 10/ 0 8/1999 First interim analysis by independent DSMB (Efficacy stopping rules based on method of O’Brien - Fleming) Recommendation: “Continue the trial” 6/28/2000 Second interim analysis by independent DSMB Recommendation: “Stop trial for highly statistically significant results” 7/26/2000 Last patient enrolled completes study Timeline of Study W. Macias, Eli Lilly
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
W. Macias, Eli Lilly Primary Analysis Results2-Sided p-Value 0.005Relative Risk Reduction 19.4%Absolute Risk Reduction 6.1% (NNT=16) 35 30.8% 30 24.7% 25 20 15 Drotrecogin Alfa (activated) (N=850) Placebo (N=840) 10 5 0 28 day Mortality
100 90 Drotrecogin Alfa (activated) (N=850) 80 Percent Survivors Placebo (N=840) 70 p=0.006 (stratified log-rank test) 0 0 7 14 21 28 Days from Start of Infusion to Death Survival Analysis (Intention to treat) W. Macias, Eli Lilly
Drotrecogin Alfa N (activated) Placebo Overall 1690 24.7 30.8 1st Quartile 433 15.1 12.1 2nd Quartile 440 22.5 25.7 3rd Quartile 366 23.5 35.8 4th Quartile 451 38.1 49.0 0.7 1.25 0.5 1.67 0.8 0.9 0.6 1 2 Relative Risk of Death (Point Estimate and 95% CI) PROWESS: Mortality by APACHE II Quartile W. Macias, Eli Lilly
15 10 5 Drotrecogin Alfa 0 (activated) (N=770) -5 Median Percent Change from Baseline Placebo (N=729) * -10 * * * p<0.05 -15 * -20 * -25 * -30 * Pre- 1 2 3 4 5 6 7 infusion Study Day PROWESS Study: D-DimerPercent Change from Baseline W. Macias, Eli Lilly Treatment groups compared using ranked ANOVA.
PROWESS Study: Thrombin-Antithrombin Complex – Percent Change from Baseline W. Macias, Eli Lilly Treatment groups compared using ranked ANOVA
RPOWESS Study: Plasminogen Activator Inhibitor-1 – Percent Change from Baseline Treatment groups compared using ranked ANOVA W. Macias, Eli Lilly
PROWESS Study: Interleukin-6 Change from Baseline Treatment groups compared using ranked ANOVA W. Macias, Eli Lilly
Xigris (Drotrecogin Alfa (activated)) Approved in United States with the Following Indication Statement: • Xigris is indicated for the reduction of mortality in adult patients with severe sepsis (sepsis associated with acute organ dysfunction) who have a high risk of death (e.g., as determined by APACHE II score, see Clinical Trial Section). • Efficacy has not been established in adult patients with severe sepsis and lower risk of death. • Safety and efficacy have not been established in pediatric patients with severe sepsis. W. Macias, Eli Lilly
Intensive DOCTOR care • Time to take a breath…
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
Reference Diseases • Incidence in US (cases per 100,000) • Colon cancer 50 • Breast cancer 110 • AIDS 17 • Congestive heart failure ~130 • Sepsis ~300 • Number of deaths in US each year • Acute myocardial infarction 211,000 • Severe sepsis 215,000 Slide presentation, D. Angus, SCCM 2001
Hospital costs associated with sepsis • Average hospital LOS - 19.6 d • Average hospital cost - $22,100 • National costs - $16.7 billion • Neonates - $1.1 billion • > 65 yrs - $8.7 billion Slide presentation, D. Angus, SCCM 2001
Resolution of organ failure • Patients treated with APC had quicker resolution of: • Cardiovascular failure • Respiratory failure • Patients treated with APC had more • vasopressor-free days (20.06 versus 18.78 days, p=0.014) • ventilator-free days (14.33 versus 13.24 days, p=0.049)
http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/http://www.fda.gov/ohrms/dockets/ac/01/slides/3797s1_02_Forsyth/
Functional status • No difference in independent ADLs • Bathing • Dressing • Toilet care • Transferring • Continence • Feeding
Hospital costs/resources • For survivors and non-survivors, use of APC did not increase: • Hospital and ICU length of stay • TISS points • Estimated costs (not including drug) Clermont et al., AJRCCM 163(5):A802
Cost effectiveness/utility • $27,400/QALY (High risk)—Angus • $46,560/QALY vs. $32,872 (High risk)—Manns • CDN$67,700/QALY vs. CDN$31,500/QALY (High risk)--Coyle
Autologous BMT for relapsed Hodgkins Adjuvant tamoxifen in premenopausal ER- women Dialysis for ESRD ICD vs. amiodarone Xigris vs. standard of care (high risk) $421,000 $57,000-$214,000 $40,000 $27,400-$32,900 $23,000 Health economics
Conclusions • Long-term follow up? • Cost-effectiveness analysis will have to take into account: • Money saved by health care system • Benefits to quality of life (cost-utility analysis) • Comparison to other public health problems/solutions • Compare/combine with other therapies? (e.g., steroids) • Await results of randomized trial in severe sepsis patients with low severity of illness scores


![Biologics License Application: Recombinant Human Activated Protein C (rhAPC) [drotrecogin alfa (activated)] Xigris ™ f](https://cdn0.slideserve.com/1354659/slide1-dt.jpg)