Download
1 / 19
260 likes | 588 Views
The stubborn platelet - rEFRACTORINESS AT ITS WORST. Dr. Anila Mathan, Consultant, Blood Bank & Hematology, SRM Institute of Medical Sciences , Chennai. Platelet transfusion refractoriness . Clinically suspected when patients do not respond as expected to the transfusion

E N D
The stubborn platelet -rEFRACTORINESS AT ITS WORST Dr. Anila Mathan, Consultant, Blood Bank & Hematology, SRM Institute of Medical Sciences , Chennai
Platelet transfusion refractoriness • Clinically suspected when patients do not respond as expected to the transfusion • Definition* :When 2 consecutive platelets transfusions lead to a 1 hour post transfusion Corrected Count Increment (CCI) of less that 5000 platelets per m2 per µl. • Average expected increment • 1 unit of random platelets 5000-10,000/cumm • 1 unit of apheresis platelets 30,000-60,000/cumm • If pre & post transfusion platelet counts are not appropriately tested the diagnosis is unlikely to be made *AABB 16thEdn
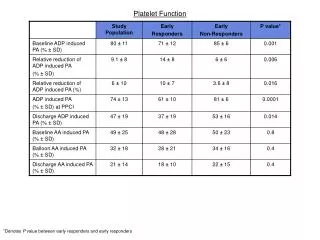
Guidelines for assessment of Platelet Refractoriness • Pre transfusion count to be done just prior to transfusion. • Post transfusion platelet count to be done1 hour & 18-24 hrs after transfusion to calculate Absolute Count Increment(ACI) or CCI. • The clinical response of the patient to the transfusion by cessation of bleeding is an important indicator for further tests. • Norms for our population are not yet established
AABB , Technical manual 16thEdn Pavenski et al, Tissue antigens 2012 BSA = Body surface area
PLATELET REFRACTORINESS Poor response to platelet transfusions Immune Causes (20%) Non Immune Causes (80%) Alloimmune Autoimmune Patient Related Platelet Related ABO incompatibility Fever , Sepsis Quality of platelets Splenomegaly HLA Class 1(80-90%) Number of units Tx DIC Poor storage condition Human platelet antigen (10-20%) Active bleeds Dilution by blood volume HLA & HPA (rare) Drugs (Egamphoterecin B
Platelet Antigens HLA ABH 8 weeks Class1 , IgG No dose response HPA
Evaluation • HLA Matching /Typing : Class 1 • Screening for anti-HLA and anti-platelet antibodies • Antibody-mediated or not? Solid-phase assay • HLA antibody mediated or not? Panel reactive antibody (PRA) as general screen for HLA Ab positivity. (20-30%) • Flow based assays :If positive, single antigen testing with microparticle beads to ID which antigen(s) to avoid in donors • Luminex based single antigen bead assay • C1q based SAB binding assay – better method for clinically relevant HLA abs (Fontaine etal,2011)
Slichter SJ. Evidence-Based Platelet Transfusion Guidelines Hematology 2007 • Platelet crossmatching can used to check compatibility • Platelet unit segment against patients serum • Solid-phase red cell adherence (SPRCA) test most widely used method • Disadvantage : • Limited to units available for testing • 5 day life to platelets, future transfusions will require re-crossmatching • Used in Europe and US as an alternative to HLA matching
Prevention • Non Immune • Blood Bank role • Clinicians role • Immune • ABO compatible • HLA to ensure compatibility • HPA • ABO compatibility • Ensure donor recipient ABO compatibility • Rate of platelet refractoriness is 69% in ABO incompatible transfusions while in ABO compatible transfusion it is only 8%
Reduction of alloimmunisation Recipient Transfusion product • IVIG, Cyclosporin • Plasmapheresis Prophylactic single donor platelets Only HLA matched plts Leukoreduced platelets Irradiated platelets Pavenski et al, Tissue antigens 2012 • Decrease in alloimmunisation from 45% to 17-21% in previously unexposed patients – LR & UVB irradiation (TRAP study , NEJM 1997) • Universal prestorageleukoreduction incidence drop :Adopted in 19 countries
Management • ABO matched platelet (<48 hrs old) • HLA matching • Challenge in obtaining a well matched donor • HLA typed donor registry • Identify HLA antibody specificities and select antigen compatible donors • Degree of matching is important • Cross reactive groups (CREGS) • 2006 HLA matchmaker (software tool) - adequate CCI • Recently 2010 epitope based matching • PRA • Platelet cross matching • Whatever the methodology for matching • Requires a large pool of dedicated typed donors • No guarantee of a proper increment • Not suitable for urgent requirements
Whatever the cause • Cost of managing a refractory patient is very high (Meehan et al Am J Hematol 2000 ;64:251-6) • How do we advice or manage a persistently refractory patient • Small dose frequent platelet transfusion every 4-8 hrs • This maintains vascular integrity even if the CCI does not increase • IVIG • Fibrinolytic inhibitors to stabilise any clots formed • Recombinant factor VIIa to control bleeding Slichter SJ. Evidence-Based Platelet Transfusion Guidelines Hematology 2007
Indian scenario • Pubmed showed that studies have been reported in 4 tertiary care centre • The reports do not differ significantly from studies in the west. • However this a condition which we need to keep in mind especially in patients requiring multiple transfusions. Shastry S, ChaudaharyR,Clinical factors influencing corrected count increment. Trans Ap Sc, 2012, MarwarhaN,Sharma RR, Consensus and controversies in platelet transfusion.TransAp sc2009 41(2) Bajpaietal. Platelet alloimmunization in multitransfused patients with haemato-oncologicaldisorders,TransAp Sc2012, Pandey p etal 2012 A prospective quality evaluation of single donor platelets (SDP) - an experience of a tertiary healthcare center in India., Chodhry VP Platlet therapy ,IJP 2002 69(9)
Conclusion • Always suspect refractoriness if patients symptoms or platelets counts don’t improve. • Try to ensure ABO compatibility . • Universal Leukodepletion seems to be one solution . • Crossmatched compatible platelets seem to be another. • Cost effectiveness of all approaches to this problem is a challenge.
Communication, Coordination,Logistics are the key to the success of any enterprise including tackling the stubborn platelet Thank you