Download
1 / 50
510 likes | 685 Views
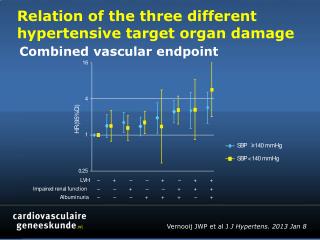
End Organ Damage- The Kidney. JogiRaju Tantravahi, M.D. Nephrology Fellowship Training Program Director Division of Nephrology University of Florida College of Medicine Staff nephrologist , Malcom Randall VA Medical Center. Disclosures of Financial Relationships.

E N D
End Organ Damage-The Kidney JogiRaju Tantravahi, M.D. Nephrology Fellowship Training Program Director Division of Nephrology University of Florida College of Medicine Staff nephrologist, Malcom Randall VA Medical Center
Disclosures of Financial Relationships This speaker has no significant financial relationships with commercial entities to disclose. This speaker will not discuss any off-label use or investigational product during the program. This slide set has been peer-reviewed to ensure that there are no conflicts of interest represented in the presentation.
Outline • The spectrum of renal disease in HIV infection • The management of chronic kidney disease • Current methods for measuring renal function • Preserving renal function • Managing the complications of chronic kidney disease • Kidney transplantation in HIV infection • Tenofovir (Viread®) nephrotoxicity
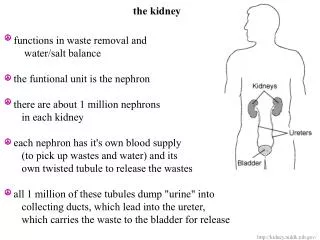
The nephron…and there’s no need to complicate things. Blood goes in Filtrate of plasma made in the glomerulus Blood comes out The filtrate of plasma is reabsorbed and modified throughout the nephron. Modified from brutal internet artwork
So how do you know that the patient has a kidney problem (and we’ll see this slide again)? • Elevated creatinine or a reduced calculated GFR • Electrolyte abnormalities, such as hyperkalemia, metabolic acidosis, or hyperphosphatemia • Abnormal urinalysis, with hematuria, pyuria, proteinuria, or casts • Decreased urine output or edema
Causes of chronic kidney disease in the HIV population I cannot find significant fault with the spectrum of kidney diseases in patients with HIV disease outlined by the authors. However, in considering the causes of renal disease in the current HIV population, I suggest that more gain will be made if we focus on managing the routine causes of chronic kidney that wee see in the general population *such as diabetes and hypertension), as I believe that the routine causes chronic kidney have or will become more prevalent than the exotic causes. When I now see chronic kidney disease patient with HIV, I ask how well has the disease been controlled, what drugs does the patient take, and if the patient has diabetes or hypertension. Elewa, U. et a. 2011 NephonClinPrac118: 346-354
Normal glomerulus and collapsing glomerulopathy of HIV associated nephropathy Global sclerosis seen in a glomerulus in a patient with the collapsing glomerulopathy of HIV associated nephropathy. Note that the entire tuft is involuted with no open capillaries with likely mesangial cell proliferation. The capillaries in the glomerular tuft are open, allowing for glomerular filtration. Obsolescent glomerulus Thin, attenuated tubules The cell number is appropriate. Dilated tubules with microcysts and proteinaceous casts Normal glomerular structure, from H. Rennke, UpToDate Wyatt, C.M, Meliambro, K., and Klotman P.E. 2012 Ann. Rev. Med. 63: 147-159
Kidney disease screening algorithm Estrella, M.M., and Fine D. M. 2010 Adv Chronic Kid Dis17: 26-35
Clinical concepts and entities you need to understand and manage
So how do you know that the patient has a kidney problem (and here’s the slide again)? • Elevated creatinine or a reduced calculated GFR • Electrolyte abnormalities, such as hyperkalemia, metabolic acidosis, or hyperphosphatemia • Abnormal urinalysis, with hematuria, pyuria, proteinuria, or casts • Decreased urine output or edema
My chronic kidney disease management paradigm • FIGHT FOR EVERY NEPHRON! • Measurements of renal function • The stages of chronic kidney disease • The consequences of chronic kidney disease and their management • Hypertension • Anemia • Bone and mineral metabolism • Electrolyte abnormalities • When things fail…replacement therapy with dialysis or transplantation
Serum creatinine • a surrogate marker for renal function • normal range typically 0.6 mg/dl to 1.1 mg/dl • higher values indicate worse renal function. • Problems equating elevated creatinine with renal dysfunction • Muscular people • Large muscle mass • Higher creatinine with normal renal function • Emaciated people • Low/no muscle mass • Falsely low creatinine in face of renal dysfunction
Ways to measure renal function, I • 24 hour urine • You need an adequate collection • Men should excrete between 15 mg/kg to 20 mg/kg of creatinine daily • Women should excrete between 10 mg/kg to 15 mg/kg creatinine daily • In near end stage renal disease, creatinine secretion is increased, so you need to measure the urea clearance as well and average the values
Ways to measure renal function, II • Cockroft-Gault formula • CrCl (ml/min)= (140-age) x lean body weight (kg) PCr (mg/dl) x 72 • MDRD formula • 170 x [Cr]-0.999 x [BUN]-0.170 x [Alb]0.318 x Age-0.176 x 0.762 (Female) x 1.180 (African American) • CKD-EPI formula • GFR = 141 X min(Scr/κ,1)α X max(Scr/κ,1)-1.209 X 0.993Age X 1.018 [if female] X 1.159 [if black] where Scr is serum creatinine (mg/dl), κ is 0.7 for females and 0.9 for males, α is –0.329 for females and –0.411 for males, min indicates the minimum of Scr/κ or 1, and max indicates the maximum of Scr/κ or 1. • Cystatin C, iothalmate clearance MDRD formula: Levey , A.S.et al. 2006 Ann Int Med 145: 247-254 CKD-EPI formula: Levey, A.S. et al. 2009 Ann Int Med 150: 604-612
Ways to measure proteinuria • Urinary dipstick • Imprecise and not quantitative • 24 hour urine collection • The collection has to be well done, or the result cannot be interpreted. • Spot urine for protein and creatinine • The lab reports the value as mg protein/gram creatinine. Since we generally excrete 1 gram creatinine daily, the spot urine ratio is generally reliable. • Albuminuria, tubular proteinuria vs. light chains • Role of the urinary albumin to creatinine ratio, serum and urine protein electrophoresis, serum free light chains
Communicating with your nephrologist:Stages of chronic kidney disease • Stage I: Normal GFR (greater than 90 ml/min) and persistent albuminuria • Stage II: GFR between 60 ml/min and 89 ml/min and persistent albuminuria • Stage III: GFR between 30 ml/min and 59 ml/min. • Stage IV: GFR between 15 ml/min and 29 ml/min. • Stage V: GFR less than 15 ml/min or end stage renal disease. As formulated by the National Kidney Foundation
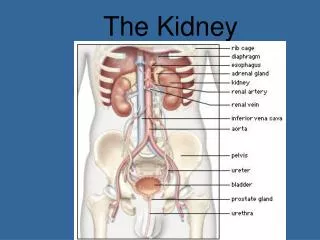
What does the kidney do? • The major homeostatic organ • Electrolyte balance, acid-base balance, salt and water balance • Detoxification and drug metabolism • Organic acids, renal excretion of drugs • An endocrine organ • Terminal hydroxylation of vitamin D, erythropoietin synthesis • Glomerular filtration and reclamation
The incredible absorptive capacity of the kidney SubstanceFilteredExcreted% net reabsorbed Water 180 liters 0.5-3 liters 98-99% Sodium 26,000 mEq 100-250 mEq >99% Chloride 21,000 mEq 100-250 mEq >99% Bicarbonate 4,800 mEq 0 100% Individuals with a normal GFR essentially can conserve all the sodium, water, and bicarbonate filtered at the glomerulus. However, fine hormonal control allow us to excrete sodium, water, or even bicarbonate. Additionally, the kidneys are efficiently excrete potassium in a response to a potassium load.
The consequences of chronic kidney disease • Beyond the devastating effects of the loss of renal function in an of itself, chronic kidney disease is accompanied by a number of devastating complications. • Cardiovascular disease • Hypertension (including volume overload) • Anemia • Bone disease • Protein malnutrition not related to cachexia • Electrolyte abnormalities • Metabolic acidosis
General principles regarding the management of chronic kidney disease • Hypertension control (target systolic blood pressure of 130 mm Hg or less) using renin-angiotensin system blockade (ACE inhibitor, angiotensin receptor blocker, mineralocorticoid receptor blocker, direct renin antagonist) • Diabetes control (target HbA1c of 7.0% or less) • Lipid control (target LDL of in the 70 range or a 20% reduction from baseline) Summary of several trials, including UKPDS, IDNT, REIN I and II, RENAAL
Cardiovascular complications of chronic kidney disease • Accelerated atherosclerotic coronary disease • Left ventricular hypertrophy • Increased prevalence of sudden death (especially in the end stage renal disease population) • Medial coronary artery calcification
Renin-angiotensin system blockade: The mainstay of hypertension management in my practice • Clinical trials support the widespread use of renin-angiotensin system blockade for hypertension therapy and renal function preservation. • Collaborative Study Group • UKPDS • RENAAL Trial • IDNT Trial • REIN Trials (both REIN I and REIN II) • HOPE Trial
You have to be brave • Renin-angiotensin system blockade abrogates the loss of renal function and prevents cardiovascular mortality. • Expect a modest increase in the creatinine • Tolerate up to a 25% increase in the creatinine as long as the blood pressure comes under control. • Risk of hyperkalemia exists • Manage with potassium lowering drugs rather than stopping the drug • Risk of cough or angioedema
Hypertension and chronic kidney disease • Multi-modal therapy is required • Polypharmacy is the rule, not the exception • ACE inhibitor • Angiotensin receptor blockers • Diuretics (loop and thiazide) • Sympathetic blockade • Calcium channel blockers (non-dihydropyridines in patient with proteinuria) • Aldosterone antagonists • Other second line drugs (clonidine, hydralazine, minoxidil, direct renin antagonists)
The ONTARGET studies • ONTARGET: Telmisartan, ramipril, or both in patients at high risk for vascular events. • NEJM 2008 358: 1547-1559 • “Renal” ONTARGET: Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): a multi-center randomized, double blind controlled trial. • Lancet 2008 372: 547-553
The bottom line • Dual renin-angiotensin system blockade might worsen renal disease, especially in patients without proteinuria. • I will use dual renin-angiotensin blockade, but mainly in patients with proteinuria (greater than 1 g protein/gram creatinine) and only as a last resort in patients without proteinuria.
Common electrolyte abnormalities seen in the outpatient setting • Hyperkalemia • (you’ll need to manage this) • Metabolic acidosis • (you’ll need to manage this) • Hyperphosphatemia • (not really your problem) • Hypocalcemia • (only your problem if the patient has symptoms like paresthesias)
Hyperkalemia, I • Potassium value greater than 5.0 mEq/l. • Patients who are in a steady state with modestly elevated potassium are usually in no danger. • However, hyperkalemia can be a silent killer and should not be ignored. • Main symptom of hyperkalemia is profound weakness with arrhythmia as the mode of death
ECG findings in hyperkalemia The ECG shows stereotypical findings including a first degree AV block, a widened QRS, and a ”sine wave” pattern in the terminal state. http://www.merckmanuals.com/professional/endocrine_and_metabolic_disorders/electrolyte_disorders/disorders_of_potassium_concentration.html
Hyperkalemia, II • Causes • Decreased GFR • Drugs • ACE inhibitors, ARBs, beta-blockers • Diet • Treatment • Dietary restriction • Diuretic therapy (mainly loop diuretic therapy) • Daily low dose sodium polystyrene sulfonate (Kayexelate®) • Modification of drug regimen
Metabolic acidosis, I Where a metabolic acidosis defined as a bicarbonate level less than 22 mEq/l.
Bicarbonate treatment of metabolic acidosis protects against deterioration of renal function de Brito-Ashurst, I., et al. 2009 JASN 20: 2075-2084
Clinical concepts you need to understand but not necessarily manage
Anemia: The causes • Decreased red blood cell half-life (important) • Malabsorption of iron and folate (important) • Chronic bleeding related to platelet dysfunction from uremia (not important) • Severe hyperparathyroidism (not important) • Erythropoietin deficiency • (very important)
As the GFR falls, anemia worsens 15 14 13 12 11 Mean Hgb* (g/dL) 10 9 8 7 6 5 n = 59 n = 29 n = 18 n = 18 n = 34 n = 18 91 90–40 39–30 29–20 19–10 10 GFR (mL/min/1.73 m2) Adapted from Foley, R.N., 2002 ClinNephrol58 Supp 1: S58-S61.
Anemia management in chronic kidney disease • Rule out iron deficiency anemia, determine the cause if presents, and restore iron stores • Rule out folate or B12 deficiency • Use an erythropoiesis stimulating agent • Erythropoietin-alpha (Procrit®) or darbepoietin (Aranesp®) in pre-ESRD • The results from several well done trials (CHOIR, CREATE, TREAT) in pre-ESRD patients have shown that the target hemoglobin should fall between 10 g/dl and 11 g/dl. Normalization of the hemoglobin should not be the goal. CHOIR: Singh, A.K., et al. 2006 NEJM 355: 2085-2098. CREATE: Drueke, T.B. et al. 2006 NEJM 355: 2071-2084 TREAT: Pfeffer, M.A., et al. 2009 NEJM 361: 2019-2032.
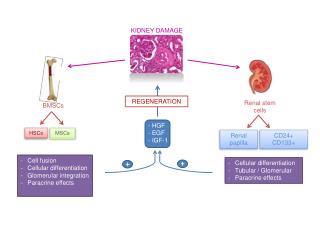
Vitamin D synthesis and feedback loops (simplified) Too much: Inhibits (parathyroid hormone) PTH gene transcription Too little: Induces PTH gene transcription The fewer nephrons available, the less efficiently terminal hydroxylation of 25- hydroxycholecalciferol occurs.
Bone disease (or why we’re so obsessed with phosphate binders) • In Chronic Kidney Disease: • Active vitamin D is not made because of decreased 1-a-hydroxylase activity. • Phosphorus levels rise because of the decreased GFR • Decreased vitamin D levels and hyperphosphatemia increase PTH levels, and the increase in PTH activity starts several seemingly beneficial compensatory processes.
Pathophysiological networks in secondary hyperparathyroidism Decreased GFR Hyperphosphatemia Metabolic acidosis Decreased vitamin D synthesis FGF 23 resistance Secondary Hyperparathyroidism Hypocalcemia Decreased calcium sensing receptor occupancy Osteitisfibrosa ...with involution of the bone marrow space
Bone disease, I • Treatment begins with lowering the phosphate level. Our options include: • Non-calcium containing binders: • Sevelamercarbonte (Renvela®) 800 mg • Lanthanum carbonate (Fosrenol®) 500 and 1000 mg • Aluminum hydroxide (Amphojel®), which should essentially never be used • Some iron based phosphate binders are in preparation • Calcium containing binders • Calcium carbonate (TUMS®) • Calcium acetate (PhosLo®and PhosLyra®) 667 mg
Bone disease, II • The NKF, through K/DOQI, has established the following PTH goals: • Stage III chronic kidney disease: GFR between 30 ml/min and 59 ml/min: • Target PTH should be between 30-70. • Stage IV chronic kidney disease : GFR between 15 ml/min and 29 ml/min. • Target PTH should be between 70-110. • Stage V chronic kidney disease: GFR less than 15 ml/min or end stage renal disease or end stage renal disease. • Target PTH should be between 150-300.
Bone disease, III • Vitamin D and vitamin D analogues directly inhibit expression of the PTH mRNA. The options include: • 1,25-dihydroxy-vitamin D (Calcitriol®, or Rocaltrol®) • 19-nor-1,25-dihydroxy-vitamin D2 (Paricalcitol®, or Zemplar®) • 1-a-hydroxy-vitamin D2 (Doxercalciferol®, or Hectorol®) • Only one non-vitamin D PTH suppressor, cinacalcet, or Sensipar®, exists. Cincalcet binds to the calcium sensing receptor on the parathyroid gland and prevents release of PTH from storage granules. • I find little use for the calcium/vitamin D preparation or for 25-OH-cholecalciferol in advanced stage III or stage IV chronic kidney disease.
My office guidelines for chronic kidney disease management, I • Blood pressure control • Target systolic blood pressure of 130 mm Hg or less on an ACE inhibitor or ARB based regimen (which will also reduce proteinuria) • Diabetes control • Target HbA1c less than 7.0% • Lipid control • Target LDL in the 70 range or a 20% reduction from baseline (SHARP study) using statin therapy
My office guidelines for chronic kidney disease management, II • Anemia • Target hemoglobin 10 g/dl and 11 g/dl after iron stores have been repleted • Bone • Target phosphorus level below 4.5 mg/dl using phosphate binders and achieve appropriate PTH control. • Electrolytes and metabolic acidosis • Limit potassium, replace bicarbonate
When things get worse…and they will • Re-double your efforts to make sure that conservative management has been optimized and that the underlying disease states are stable. • Has a new drug been started (drug induced allergic interstitial nephritis)? • Could the patient have ureteral obstruction? • Is there a concurrent severe illness? • Discuss dialysis and transplantation.
Kidney transplantation: an option in very selected patients, I • 40 kidney transplants at a single center • CD4 count greater than 200 cells/mm3, viral load < 400 copies/ml. • Induction with basiliximab and intravenous methylprednisone and maintenance with prednisone, tacrolimus, and sirolimus (a regimen now proven to be sub-optimal). • Two year overall survival was 82%, graft survival was 71%, and acute rejection occurred in 22% of patients. • None of the patients had a reduction in the CD4 count, and no opportunistic infections were noted. By and large the HIV viral load was undectatable. Kumar, M.S. et al. 2005 Kidney Int67: 1622-1629
Kidney transplantation: an option in very selected patients, II • 150 HIV infected patients followed at 19 transplant centers transplanted between 2003 and 2009 • Patients had a CD4 count greater than 200 cells/mm3, viral load < 50 copies/ml. • Immunosuppressive regimen was modern. • 1 year patient survival was 94.6% and 3 year patient survival was 88.2% • 1 year graft survival was 90.4% (acceptable) and 3 year graft survival was 73.7% (not great). • CD4 counts did not fall, but viremia worsened in patients who received anti-thymocyte globulin induction. • But acute rejection rates were unacceptably high. Stock, P.G., et al. 2010 NEJM 363: 2004-2014
So when should you enlist the aid of a nephrologist? • Anytime you want… • Patients with stage III CKD • When the velocity of the increase in the creatinine rises above what you would expect • Blood pressure becomes more difficult to control. • Urinary protein excretion rate rises into the nephrotic or high non-nephrotic range. • Electrolyte abnormalities present or more difficult to manage.
Two slides regarding tenofovir Izzedine, H., Harris, M., and Perazella, M. 2009 Nat Rev Neph9: 563-573
Tenofovir use in chronic kidney disease • Undoubtedly, a measurable incidence of Fanconi syndrome and chronic kidney disease exists in patients receiving tenofovir. • However, a recent systematic review (Cooper, R.D. et al 2010 ClinInfDis51: 496-505) noted that the risk was small and perhaps limited to underweight patients or those with a high viral load and low CD4 count. • They did not see the need to withhold tenofovir if the drug was needed and if the renal function and electrolytes were monitored carefully.