Download
1 / 48
500 likes | 1.01k Views
Military Sports Medicine Fellowship. Return to High Altitude Activity After High Altitude Illness. “Every Warrior an Athlete”. Kevin deWeber, MD, FAAFP Director, Primary Care Sports Medicine Fellowship. Objectives. Review pathophysiology of high altitude illness (HAI)

E N D
Military Sports Medicine Fellowship Return to High Altitude Activity After High Altitude Illness “Every Warrior an Athlete” Kevin deWeber, MD, FAAFP Director, Primary Care Sports Medicine Fellowship
Objectives • Review pathophysiology of high altitude illness (HAI) • Review the types of HAI and how they are treated • Review factors predisposing to HAI • Discuss preventive treatment for those with a remote history of HAI • Discuss factors in return-to-altitude decisions after recent HAI
Preview • Little evidence for recommendations of return to altitude activity after HAI • Acclimatization and slow ascent are powerful • Ascend < 600 m/day • Rest day every 600 – 1200 m • Prophylactic meds advised if unable to comply • Consider neuro-psych deficits from moderate AMS/HACE and their effect on activity
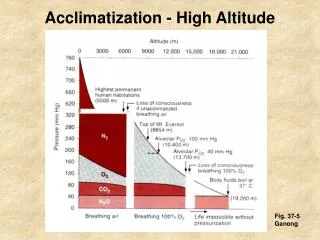
Environment at high altitude(>1500 m or 4920 ft) • Barometric pressure decreases • Partial pressure of oxygen decreases • RESULT: “Hypobaric Hypoxia” • Lower alveolar O2 leads to lower SaO2
Ft. Carson, CO, ~6500 ft Pikes Peak, 14,110 ft (4300 m) US Air Force Academy, ~7,000 ft
Acclimatization • Immediate (minutes to hours) • ↑ Sympathetic tone ↑ HR & CO • ↑ Ventilation ↑ PaO2 and↓ PaCO2 ↓ pH • Renal bicarbonate diuresis (to balance pH) • ↑ Pulmonary artery pressure ↑ O2 absorption • Delayed (days to weeks) • Erythropoietin ↑ RBC production • Remodeling of pulmonary arterioles
Altitude Illnesses (Failure to Acclimatize) • Cerebral Syndromes • Acute Mountain Sickness (AMS) • High Altitude Cerebral Edema (HACE) mild AMS moderate AMS HACE • Pulmonary Syndrome • High Altitude Pulmonary Edema (HAPE) • Importance • HACE and HAPE can be fatal
Acute Mountain Sickness(AMS) • Defined as HEADACHE plus one or more symptom: • Anorexia, nausea or vomiting • Fatigue or weakness • Dizziness or lightheadedness • Difficulty sleeping
Effects of AMS on performance • Mild: annoyance only • Moderate: impaired concentration, memory, speech, and physical performance; • Can be disabling • Subtle abnormalities visible on MRI • Effects can last weeks
High Altitude Cerebral Edema(HACE) • AMS symptoms plus ALTERED L.O.C. and ATAXIA • Other neuro findings possible • Coma develops • Death results if untreated • Pathophysiology • altered cerebral vascular permeability leads to brain swelling • MRI: cerebral edema, lesions of corpus callosum
High Altitude Pulmonary Edema(HAPE) • Defined by two pulmonary symptoms… • Cough, dyspnea at rest, exercise intolerance, chest tightness/congestion… • and two pulmonary signs… • Crackles, wheezing, cyanosis, tachypnea, tachycardia • Most common cause of death among HAI • 50% mortality rate if not treated quickly
High Altitude Pulmonary Edema(HAPE) • CXR findings • Blotchy fluffy infiltrates • Pathophysiology Hypoxia pulmonary artery hypertension • alveolar damage edema and hemorrhage into alveoli
Risk factors for HAI • Rapid gain in altitude • Prior history of HAI • genetic factors involved • Alcohol, sedatives • HAPE: cold ambient temperature • Strenuous exercise
HAI Protective Factors • Residence at elevation >900 m (2950 ft) • Slow gain in elevation • <600 m (1970 ft) per day in sleeping elevation • Genetic factors • Vigorous fluid intake • Physical fitness NOT protective
Treating HAI • Rest, halt ascent • Descent • Moderate AMS: >500 m (1640 ft) • HACE: > 1000 m (3280 ft) • HAPE: 500 – 1000 m • Oxygen if available • Keep warm (esp. for HAPE) • Portable hyperbaric chambers
Portable Altitude Chamber® (PAC) Gamow® bag Certec® bag
Treating HAI (cont.) • Acetazolamide • Speeds acclimatization • 75% effective in preventing AMS • Treats moderate AMS & HACE • Dose: 125-250 mg BID
Treating HAI (cont.) • Dexamethasone • Decreases cerebral edema • Treats moderate AMS and HACE • Prevents AMS, ? HACE • Dose • 2 mg po/IM/IV QID • 4 mg BID
Treating HAI (cont.) • Nifedipine • Decreases pulmonary artery pressure • Prevents and treats HAPE • Dose: 20 – 30 mg extended release BID
Treating HAI (cont.) • Salmeterol • Decreases alveolar fluid transport • Prevents and treats HAPE • Dose: 125 mcg inhaled BID
Considerations for Return to Altitude Activity after HAI • Severity and type of prior HAI • Future ascent requirements • Feasibility of descent/extra rest days if needed • Availability of medical treatments
Two scenarios for Return to Altitude Activity after HAI • Remote history of HAI, fully recovered • Recent HAI, with/without recovery
1. Remote history of HAI, fully recovered • Proper acclimatization protocols are paramount • Ascend no more than 600 m (1970 ft) per day in sleeping altitude when >2500 m (8200 ft) • Spend one extra night every 600-1200 m (1970 – 3937 ft) • Avoid abrupt ascent to >3000 m (9843 ft) • Spend 2-3 nights at 2500-3000 m before ascending further
“Acute mountain sickness: influence of susceptibility, preexposure, and ascent rate” Schneider M et al. Med Sci Sports Exerc 2002
Prevention of recurrent AMS • Proper acclimatization, slow ascent. If not possible… • Acetazolamide 125-250 mg po BID starting 1 day prior to ascent, continuing until at max altitude for 2 days. If not possible… • Alternate: Dexamethasone 2 mg po QID or 4 mg BID, starting 1 day prior, cont. until at max altitude 2 days • Unknown which is better or if combination therapy is indicated
Prevention of recurrent HACE (No evidence-based recommendations) • Strong recommendation for acclimatization and slow ascent. If not possible, or descent/medical treatment not possible… • Prophylaxis with acetazolamide or dexamethasone, as for AMS
Prevention of recurrent HAPE • The power of slow ascent: case series • 4 climbers with history of 2-4 prior cases of HAPE each • Made a collective 7 ascents to > 5000 m (16,400 ft) • Acclimatized fully • Ascended only 330-350 m (984-1150 ft) a day • RESULT: no cases of HAPE (100% effective) Bärtsch P et al. High altitude pulmonary edema. Respiration 1997
Prevention of recurrent HAPE(cont.) • The power of meds: 1 R, DB, PC trial comparing prophylactic meds • Dex 8 mg bid • Tadalafil 10 mg bid • Dex & tad vs placebo: • P < 0.001 & < 0.007 • Dex vs tab: not sig • Both dex & tad reduced pulmonary artery pressure
Prophylaxis for recurrent HAPE • Strong recommendation for acclimatization and slow ascent. If not possible, or descent/medical treatment not possible… • Prophylactic options: • Tadalafil 10 mg po bid • Dexamethasone 8 mg po bid • Acetazolamide 125-250 mg po BID • Salmeterol 125 mcg inhaled BID • Nifedipine 20-30 mg XR BID • All beginning 1 day before ascent No evidence of superiority of one agent or risks/benefits of combination therapy
2. Return to Altitude Activity after Recent HAI • Considerations (same as remote HAI hx) • Severity and type of prior HAI • Future ascent requirements • Feasibility of descent/extra rest days if needed • Availability of medical treatments • Additional considerations for recent HAI • Should the patient fully recover before returning to altitude/activity? • How safe is continued activity at altitude? • Should activities be limited?
Treatment of Mild AMS • Descend > 500 m (1640 ft) OR • Rest 1-2 days at same altitude • Oxygen 12-24 hours, if available • Consider acetazolamide 125-250 mg po BID • Symptomatic treatment with analgesics, anti-emetics
Return to Altitude Activity during/after Mild AMS (No evidence-based recommendations) • Common practice: continue activity despite symptoms • Risks • Impaired cognition/performance • Progression to moderate AMS or HACE • Consider acetazolamide
“To air is human: altitude illness during an expedition length adventure race” • 10-day, 238-mile race at elevations of 9,500 – 13,500 ft • No prophylaxis allowed • 33 cases of AMS treated during race • 88% were returned to race • 58% finished race (compared to 74% overall) • CONCLUSION: untreated AMS probably reduces athletic performance Talbot TS et al. Wilderness Environ Med 2004
Treatment of Moderate AMS • Descend >500 m • Rest 1-2 days • Do not allow continued ascent/activity • Significant performance/cognition decrement • Risk of progression to HACE • Oxygen 1-2 days, if available • Acetazolamide; dex as alternate
Return to Altitude Activity after recovery from Moderate AMS (No evidence-based recommendations) • Strict adherence to acclimatization and slow ascent protocols • Ascend no more than 600 m/day • Rest day every 600 – 1200 m • Consider acetazolamide (or dex) • Counsel on recognition and rapid treatment of HACE/HAPE
Treatment of HACE • Immediate descent > 1000 m and hospitalize • Oxygen to maintain SaO2 >90% • Dexamethasone—8 mg PO/IM/IV initially followed by 4 mg QID • Portable hyperbaric therapy if descent impossible
Treatment of HACE (cont.) • Management of coma • Bladder catheterization • Airway control • Diagnostic studies • CXR to rule out concurrent HAPE • MRI to rule out other conditions
Recovery from HACE:highly variable • 1-3 days for symptoms to resolve • Days to 12 weeks for neuropsychological function to normalize • 3-4 weeks for papilledema to resolve • Days to 5 weeks for MRI to normalize
Return to Altitude Activity after recovery from HACE (No evidence based recommendations) • Full recovery highly advised • Strict adherence to acclimatization and slow ascent protocols • Ascend < 600 m/day • Rest day every 600 – 1200 m • Consider prophylaxis • Acetazolamide; dex as alternate
Treatment of HAPE • Immediate descent 500-1000 m • Oxygen to keep SaO2 >90%. • If descent/O2 not immediately available… • Portable hyperbaric therapy • Nifedipine 20-30 mg extended release BID (avoid if concomitant HACE) and/or… • Salmeterol 125 mcg inhaled
Treatment of HAPE (cont.) • Admit if: • >4L/min O2 requirement • Elderly, very young • Concomitant HACE or co-morbid cardio-pulmonary disease • Dexamethasone if concomitant HACE • Low-flow outpatient O2for others; check daily
Recovery from HAPE • Variable; little evidence in literature • May take 2 weeks to recover strength • Resume some activity when SaO2 > 90% without supplemental O2 • Remaining at some altitude fosters acclimatization via pulmonary arteriolar remodeling
“Reascent following resolution of high altitude pulmonary edema (HAPE).” • Case reports of 3 mountaineers with HAPE • Treated with… • descent to lower altitude • oxygen • rest 2-3 days • Resumed ascent; no prophylaxis • < 600 m/day ascent; several rest days • RESULT: all reached peaks w/o HAPE • One reached summit of Mt. Everest at 8850 m (29,035 ft) Litch JA, Bishop R. High Alt Med Biol 2001 Spring;2(1):53-5
Return to Altitude Activity after recovery from HAPE (No evidence based recommendations) • Strict adherence to acclimatization and slow ascent protocols • Ascend < 300 - 600 m/day • Rest day every 600 – 1200 m • Consider prophylaxis: • acetazolamide and/or • nifedipine or salmeterol (especially if ascent will be > 600 m/day)
Review • Little evidence for recommendations of Return to Altitude Activity after HAI • Acclimatization and slow ascent are powerful • Ascend < 600 m/day • Rest day every 600 – 1200 m • Prophylactic meds advised if unable to comply • Consider neuro-psych deficits from moderate AMS/HACE and their effect on activity