Download

1 / 87
1.02k likes | 3.93k Views
Mandible Angle Fracture. 가천의과대학교 길병원 구강악안면외과 전 창 훈. Mandibular Angle Fracture. Pape et al (1983), Wald et al (1988) 23~42% of all mandible fracture Mandible Fracture pattern Direction and amount of force Presence of soft tissue bulk

E N D
Mandible Angle Fracture 가천의과대학교 길병원 구강악안면외과 전 창 훈
Mandibular Angle Fracture • Pape et al (1983), Wald et al (1988) • 23~42% of all mandible fracture • Mandible Fracture pattern • Direction and amount of force • Presence of soft tissue bulk • Biomechanical characteristics of the mandible (density and mass) • Anatomic structures creating weak area • Mandible angle fracture • Biomechanics of the mandible are associated with high incidence of postsurgical complication • Gerlach (1982), Kai Thu & Terhulzen (1985), Jackson et al (1986), Ikemura et al (1988), Ardary (1989), Iizuka et al (1991) • Iizuka (1991), Ellis (1993), Assael (1994) • Mandibular angle fractures are associated with the highest incidence of postsurgical infection of all mandibular fracture
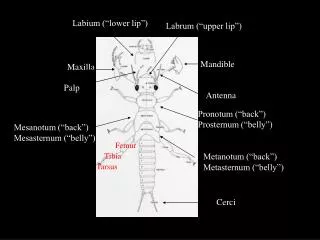
Mandibular angle anatomy • Mandibular angle is thinner than both body and ramus region • Abrupt change in shape from horizontal to vertical rami
Michielet et al (1973) • Introduce the concept of miniplate placement along the external oblique ridge for the treatment of mandibular angle fractures • Small, easily bendable noncompression bone plates, attached with monocortical screws • Champy et al (1975, 1976, 1977) • Miniplate system : ideal line of osteosynthesis, location of stable fixation • Raveh et al (1987), Luhr (1986), AO/ASIF advocates (1974) • Not feel that the plates offer adequate stabilization of the fracture to eliminate the need for IMF
Angle Fracture Treatment Methods • Closed reduction • Intra-oral OR & non-rigid fixation (wire fixation) • Extra-oral OR/IF with an AO/ASIF reconstruction bone plate • Intra-oral OR/IF using a solitary Lag screw • Intra-oral OR/IF using two 2.0 mm mini-dynamic compression plates • Intra-oral OR/IF using two 2.4 mm mandibular dynamic compression plates • Intra-oral OR/IF using two non-compression miniplates • Intra-oral OR/IF using a single non-compression miniplate • Intra-oral OR/IF using a single malleable non-compression miniplate • Intra-oral OR/IF using a biodegradable plate 1999 Int.JOMS Ellis 참고인용
Closed reduction orIntraoral open reduction & non-rigid internal fixation • Less fashionable • Transosseous wires, circum-mandibular wires, small positional plates • Postsurgical IMF : 6 weeks • Complications ; 17% • 13 infections, 4 malunion & malocclusion, 3 non-union • High incidence of postsurgical complications
Extraoral OR/IF using the AO/ASIF reconstruction plate • AO reconstruction plate is a reinforced plate that is thicker and stronger than the standard AO/ASIF compression plate • 3 screws on each side of the fracture provide adequate neutralization of functional forces in the absence of compression (Schmoker et al, 1976) • Comminuted, bone loss or obliquity (can’t use standard compression plates) • 7.5% infection, 1 patient required plate remove
Lag screws • Niederdellmann et al (1981) • Internal fixation using a single lag screw • Rapid and simple method • 17 / 88 patient unstable & supplemental fixation method • 5 patient (13%) required removal of screws and small sequestra
Intraoral OR/IF using two 2.0-mm mini-dynamic compression plates • Superior & inferior border of buccal cortex • Superior border : small compression plate with monocortical screws • Inferior border : large compression plate with biocortical screws • Extraoral approach : Not difficult • Intraoral approach : decreased visibility, difficult adaptation • 29% (9/30) complications
Intraoral OR/IF usingtwo 2.4mm mandibular dynamic compression plates • Because of the high rate of postsurgical complications in patients with two 2.0-mm mini-dynamic compression plate • Standard AO/ASIF technique by application of two compression plates specifically designed for the mandible • 2.4mm screws applied monocortically in locations where bicortical engagement would damage normal anatomy • Postsurgical suction drainage was used in all cases • 32% infections
Intraoral OR/IF usingtwo noncompression miniplates • AO/ASIF recommendation with two compression plate • High rates of complication • 2.0 mm non-compression mini-plates • Superior : monocortical • Inferior : bicortical • 28% (19/67) complications
Intraoral OR/IF using one non-compression miniplate • High rate of complication : two plate • Champy et al (1978) : one miniplate • Single 4-hole miniplate and monocortical screws • 2~4mm gap at the inferior border • 16% complications, but minor and can treated in the outpatient
Intraoral OR/IF usingone malleable non-compression miniplate • Lodde (1995) • Reduced the volume of the original champy miniplate by half • Not increased in complications • Thin, malleable miniplate (7 hole) & 1.3 mm screws (5mm) • 13.7 % complications : 8.7 % further surgical intervention • 3/7 Asymptomatic plate fracture, but bony union state • 2/7 plate fracture : mobility, 6 weeks IMF
Luhr & Hausmann (1996) • 0.9% rate of complication in 352 patients treated by compression plates for angle fracture • Ellis & Sinn (1993) • 32% rate of complication in 65 patients treated with compression plates for angle fracture • Iizuka & Lindqvist (1993) • 6.6% rate of infection and 14% rate of malocclusion for 121 angle fx
Angle fracture complication rate가 다양한 이유 (Ellis, 1999) • Angle fracture에 국한된 complication 연구가 부족하다 • Very different treatment • Vary in the etiology of the injury • Routine plate remove
Luhr (1982) • Large bone plates (usually with compression) fastened with bicortical bone screws to provide rigidity
AO/ASIF plate • Plate and screw fixation should provide sufficient rigidity to the fragments to prevent interfragmentary mobility during active use of the mandible
2 Miniplates • Levy (1991) • 2 miniplate : 3.1% complication ( superior buccal cortex, 2nd 6-hole) • Single miniplate : 20 % complication • 2 miniplate plus postsurgical IMF : • higher complication (7.1%) than no IMF • Vallenntinpo 1994 • Choi (1995) • Separation of the fracture line and lateral displacement of the proximal fragment at the lower mandibular margin • 2nd plate : inferior border • Severely disturbed biological surrounding (need for more rigid fixation) • Old, comminuted, infected or severely dislocated fracture • Edentulous mandible or with atypical tension/pressure forces due to poor dentition or pathological occlusion
1 Miniplate • Champy et al (1976) • One plate at the superior border of the mandible ventral to the external oblique line • Choi et al (1995) • Ellis (1999) • Shierle et al (1997) • Low complication rates with monocortical miniplate fixation • Michelet et al, 1973 • Champy et al, 1978 • Gerlach et al, 1983
Bio resorbable plate • Synthetic bioabsorbable materials : 30 years • Cutright and Hunsuck (1972) • Orbital floor fracture : use of resorbable materials • Bos (1989) • Attempted by using poly-L-lactide acid monomers : successful rate • But, rapid decline in tensile strength : 1 week • Eppley (1996) • Polyglycolic acid materials • 50% loss of original strength in the 2 week after placement • Total loss of the strength and consistency after 6 weeks • Combination of the 2 materials in varying ratio • Lorenz Lactosorb system • PLLA and PGA • Allow 70% of the initial strength to be retained during the first 6-8 weeks
AO/ASIF principle • Anatomic reduction • Rigid fixation • Atraumatic surgical technique • Immediate active function • 1994, AO/ASIF • Change second principle : “ functionally stable fixation ” • Single miniplate • “ neutralize ” functional forces
Mandible Fracture % • 하악골 골절 중 차지하는 비율, 성, 나이, 직업, 외상 방법? 위치 • 수술까지 경과시간, MMF 기간, 입원기간, 합병증 • 수술 접근 방법, 마취방법, 재수술여부 • 흡수성, 비흡수성, 제3대구치 잔존, 발거, 고정술 방법 • 환자의 만족도(교합), 개구장애? 저작력변화 • Question • Fractuer stability vs Infections
Complications • Champy et al (1978) • The combination of the forces of elevator muscles and occlusal forces results in a natural band of tension along the superior border in the angle region
Outcomes of Patients With Teeth in the Line of Mandibular Angle Fractures Treated With Stable Internal FixationJOMS 2002 60:863-865 Ellis • 결과 • 골절선에 치아 존재 : 85% (345/402) • 수술 동안 치아의 제거 : 75% (258/345) • 술후 감염 : 19% (75/402) 평균시간 : 8.1 weeks • P/R : 19% (75/402) • 치아와 관련없는 우각부 골절 감염율 : 15.8% • 치아와 관련된 우각부 골절 감염율 : 19.1% • 치아를 잔존시킨 경우 : 19.5% • 치아를 제거한 경우 : 19.0% • 치아와 관련없는 우각부 골절 P/R : 17.5% • 치아와 관련된 우각부 골절 P/R : 18.8% • 치아를 잔존시킨 경우 : 19.5% • 치아를 제거한 경우 : 18.6% • 결론 • 치아가 골절선에 존재하면 술후 합병증 위험이 증가하지만, 유의성은 없다. 술후 감염은 치아의 발거에 대한 문제와 연관이 없다.
Outcomes of Patients With Teeth in the Line of Mandibular Angle Fractures Treated With Stable Internal FixationJOMS 2002 60:863-865 Ellis • Angle fracture에서 술후 complication이 높은 이유 • Method of treatment • The time between injury and treatment • The oral health of the patient • Presence or absence of a tooth in the fracture line • The criteria of tooth extraction (Methods) • Fractured teeth • Pericoronal / periodontal infection • Gross caries • Tooth mobility • Exposure of the apical half or more of the root (including the apex) • Inability to reduce the fracture without tooth removal • Muller (1964) • Multirooted teeth (ie, molars) be removed • James et al (1981) • 4+ mobility, root fracture, apical pathology, not necessary for stability (39%) • Kahnberg and Ridell (1979) • 59% teeth left : clinical and radiographic sucess
Do mandibular Third Molars Alter the Risk of Angle Fracture?Fuselier, Ellis, Dodson JOMS 2002 60:514-518 • Results & Conclusions • Study sample : 1,210 patients • Patients with M3 : 2.1 times chance of angle fracture • Angulation & occlusal position of M3 : mesioangulation • Intact superior border : structural stability of the angle region • Does the removal of M3 “strength” the mandible or does it remain “weak” ? • Angle fracture incidence • Vector of force • Amout of force • Musculatrue of the face • Architecture of the mandible • M3 presence or absence
Results M3를 가진 426명 중 127명이 우각부 골절 (29.8%) M3가 없는 189명 중 25명이 우각부 골절(13.2%) Conclusions Mandibular angle that contain an impacted M3 is more susceptible to fracture Is the mandibular third molar a risk factor for mandibular angle fracture?Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000 89:143-6Ma’aita, Alwrikat M3 position & angle fx risk M3 & angle fx
Is the mandibular third molar a risk factor for mandibular angle fracture?Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000 89:143-6 • Mandible • The strongest and most rigid component of the skeleton • But, more commonly fractured than the other bones of the face • Ellis (1985) • Mandibulr angle fracture : 30% of the mandibular fractures • Wolujewicz (1980) • No relationship between the state of eruption of M3 and angle fracture • Tevepaugh and Dodson (1995) • 3.8 times more fracture with M3 • Halazonetis (1968), Amartunga (1988) • Twice occur in dentate patients compared with edentate patients • Reitzik (1978) • Unerupted M3 angle will fracture with only 60% of the force necessary to fracture the angle when the M3 is erupted
The Effect of Mandibular Third Molar Presence and Position on the Risk of an Angle FractureLee, DodsonJOMS 2000 58:394-398 • Purpose • Assessment of the relationship between M3 and angle fractures • Patients and Methods • M3 position : 9 categories (Pell and Gregory classification) • Results • Patient with M3 had a 1.9 times greater chance of an angle fx • Conclusions • M3 present have an increased risk for angle fractures (1.9 times) • M3 position is only one important risk factor
The Effect of Mandibular Third Molar Presence and Position on the Risk of an Angle FractureLee, DodsonJOMS 2000 58:394-398 • Mandibular fracture patterns • Direction and amount of force • Presence of soft tissue bulk • Biomechanical characteristics of the mandible (bone density and mass) • Anatomic structures creating weak areas • Reitzik et al (1978) • Mandible with unerupted M3s required 40% less force to be fractured than mandible with fully erupted M3 • Hypothesis • Presence of M3s decreases bone mass, thereby increasing the risk of fx • Deeper impactions increasing the risk of fracture • Huelke et al (1961,1962,1964) • Fracture occur more frequently in dentate than in edentulous • Tevepaugh & Dodson (1995) • Fail to confirm a relationship between M3 position and fracture
The Effect of Mandibular Third Molar Presence and Position on the Risk of an Angle FractureLee, DodsonJOMS 2000 58:394-398 • Deepest impacted M3s • 50% decrease in angle fracture risk • Other factors (Nahum 1975) • Soft tissue character • Remaining dentition state • Weiss (1965) • Angle region was more prone to fracture in partially or fully edentulous mandibles than in dentulous ones • Tams et al (1996) • Biomechanical property of the mandible during angle fractures • Greatest amount of positive bending moment • Small amount of torsion • Greatest amount of shear force • John et al • M3 ext or not ? Condyle fx
An investigation into the relationship between mandibular third molars and angle fractures in NigeriansUgboko British JOMS 2000 38:427-429 • Results • 65/408 with M3 (16%) vs 11/82 without M3 (13%) • Unerupted 24/77 (31%) vs erupted 52/331 (16%) • Conclusions • M3 does not necessarily predispose to fractures of the mandibular angle • But, angle fractures are more likely to occur with unerupted M3 than erupted M3 • Marker et al (1994) • Closed reduction with retention of M3 within the line of fracture carries less morbidity than rigid fixation and immediate jaw mobility
Are Mandibular Third Molars a Risk Factor for Angle Fractures? : A Retrospective Cohort StudyTevepaugh & Dodson JOMS 1995 53:646-649 • Results • 73 patient with M3, 30 angle fracture (41.1%) • 28 patient without M3, 3 angle fracture (10.7%) • Conclusions • Patient with M3 were 3.8 times more liable to develop angle fractures than those without M3 • The decreased cross-sectional area of bone associated with M3 weakens the angle • The position of the M3 does not affect the site • People at risk may benefit from pre-emptive removal of the M3
Relationship between fractures of the mandibular angle and the presence and state of eruption of the lower third molarSafdar, BMedSci, Meechan Oral Surg 1995;79:680-684 • Results • Significantly greater when unerupted M3 were present • Bilateral unerupted M3 predisposed to a fracture at the angle significantly more than unilateral unerupted M3 • Peterson (1991) • Prophylactic extraction of unerupted M3 : sports
Incompletely erupted third molars in the line of mandibular fractures ; A retrospective analysis of 57 casesMarker, Eckerdal et al Oral Surg 1994;78:426-31
Clinician variablility in characterizing mandible fracturesShetty, Atchison, Belin, Wang JOMS 59;254-261, 2001
A Biomechanical Evaluation of Mandibular Angle Fracture Plating TechniquesHaug et al JOMS 2001 59:1199-1210 • Purpose • Evaluate the biomechanical behavior of a vast array of fixation philosophies and technique • Materials and Methods • 150 polyurethane synthetic mandible replicas • Five controls and 5 each of 14 different fixation • Vertical loading at the incisal edge & contralateral loading in the molar region • Lag screw technique • Monocortical superior border plating with varying size of plates & screws • Monocortical 2-plate technique with varying forms of fixation • Monocortical tension band systems with associated bicortical stabilization plates of various types • Various forms of reconstruction plates • Conclusions • Incisal edge loading : all systems met or exceeded postoperative function • Contralateral molar loading : fail
A Biomechanical Evaluation of Mandibular Angle Fracture Plating TechniquesHaug et alJOMS 2001 59:1199-1210 • Dramatic differences in outcomes • Individual host factors • Variations in the biology of fracture healing and/or surgical technique • Biomechanical influences of the particular fixation systems • Ellis et al (1994, 1996) • Bite forces in the acute post-OP period are much less than later post-OP period or nonoperated population • Kroon et al (1991) • Different loaded torsions could displace a reconstructed fracture • Shetty et al • Adaptive systems fared less favorably than the compressive systems
Technique for Applying 2 Miniplates for Treatment of Mandibular Angle FracturesChoi et al JOMS 2001 59:353-354 • Champy method (1978) • Separation of the fracture line & lateral displacement of the fragment • Posterior open bite on the fracture side • MMF ; intraoperative and postoperative • 2-miniplate fixation • Superior border & inferior border of the mandible • Using reduction forcep : superior border fixation • Mouth prop on the contralateral molars : inferior border fixation with trocar • Advantage • No MMF : no posterior open bite • Excellent adaptation and good stability at the fracture site • Ellis et al (1992) • Unacceptably high rate of complications using 2 miniplates
Mandibular fractures in Townsville, Australia: incidence, aetioology and treatment using the 2.0 AO/ASIF miniplate systemSchon et al British JOMS 2001, 39:145-148 • Summary • 1995, 114 patient, 154 mandible fracture • 124 fracture (81%) : male, 30 fracture (19%) : female • Fight (83%), TA(10%), Falls(3%), Falling objects(3%), sport(2%) • Mn angle (43%), symphysis (26%), combine fracture (30%) • With M3 : 97% • 105 patient : 2.0 AO/ASIF titanium miniplates • Complication • Temporary sensory deficit (3%) • Minor malocclusion (2%) • Infection or dehiscence(5%) • Conclusion : 2.0 AO/ASIF miniplate system is reliable
An effective technique for open reduction of mandibualr angle fractures using new reduction forceps: technical innovationsChoi et al Int JOMS 2001, 30:555-557 • 우각부에 reduction forcep을 적용하기 힘들기 때문에 술후 complication 높을 수 있다. • Precompressing fractures는 골 접촉면적을 증가시켜서 stability와 healing에 도움이 된다. • 1 hole ; proximal fragment medial to the oblique line • 2 hole ; distal fragment below the oblique line • But, oblique surface fractures : not advised • Cause fragment overriding
Treatment of Mandibular Angle Fractures with a Malleable Noncompression MiniplatePotter & EllisJOMS 1999 57:288-292 • Purpose • Single, thin, malleable miniplate로 우각부 골절 치료를 평가 • Patients and Methods • 51 fracture : OR/IF using one noncompression, thin, malleable miniplate and 1.3mm self-threading screws • No postsurgical MMF • Results • 7 (15.2%) complication • 3 asymptomatic bone plate fracture : already heal, no treatment • 2 bone plate fracture : fracture mobility, requir MMF • 3 infection : I & D • Conclusions • Small one bone plate for angle fractures provided adequate fixation • But, unacceptable rate of plate fracture, the plate cannot be recommended for routine
Treatment of Mandibular Angle Fractures with a Malleable Noncompression MiniplatePotter & EllisJOMS 1999 57:288-292 • Single, 2mm miniplate was much fewer complication than 2 plates • Lodde (1995) • Reduced the volume of the original Champy miniplate by half • Not increased in complication • Seven-hole noncompression titanium miniplate • Six 5mm long, 1.3mm diameter self-threading screws • Unnecessary to bend • Rigid fixation • Forming a stronger bone • Little or no MMF • Earlier physical rehabilitation & function • Fracture healing factors • Minimum disruption of the periosteum and improve vascularity • Inadequate cooling of bur (bicortical) • Direction of the fracture line • Posterior molar occlusion
Treatment methods for fractures of the mandibular angleEllis Int JOMS 1999, 28:243-252 • Angle fracture가 빈번히 발생하는 원인 • The presence of third molars • A thinner cross-sectional area than the tooth-bearing region • Biomechanically the angle can be considered a “lever” area • Treatment methods : 앞 slide에 정리 함 • Most useful : AO/ASIF or single miniplate
Treatment methods for fractures of the mandibular angleEllis Int JOMS 1999, 28:243-252 • Discussion • No recommend an intraoral two-plate technique • High rate of sequestra formation, infection and need for subsequent surgery • Two point fixation was much higher than one point fixation • Single miniplate fixation • Complication was easily treated in the outpatient clinic under local anesthesia • Plate remove was simple • Shierle et al (1997) • One- or two- plate : no significant difference in results
Biomechanical evaluation of new fixation devices for mandibular angle fracturesWittenberg et al Int JOMS 1997, 26:68-73 • Mandible angle fractures : 23~42% of all mandible fractures