Download
1 / 34
340 likes | 509 Views
Psychological Approaches to Understanding & Promoting Continence. An Overview:. Behavioural Models Behavioural Interventions Effectiveness of Behaviour Therapy References and resources. A psychological perspective can help:. Understanding the psychological consequences of incontinence

E N D
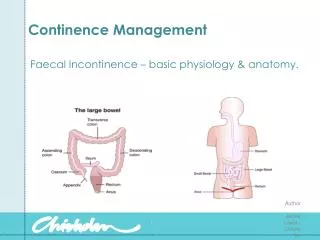
Psychological Approaches to Understanding & Promoting Continence
An Overview: • Behavioural Models • Behavioural Interventions • Effectiveness of Behaviour Therapy • References and resources
A psychological perspective can help: • Understanding the psychological consequences of incontinence • Explain continence / incontinence • Identify strategies for developing and promoting continence e.g. Behaviour Therapy
The Behavioural Perspective • Based on theories of learning • Views continence as appropriate response to stimuli and / or • A set of skilled behaviours that need to be learned (and can be taught) • Assumes behaviours can be objectively observed & measured (unlike some other models) • Various treatments can be seen to be derived from one or more approaches to learning
3 Behavioural Models • Classical Conditioning • Focus on conditioned stimuli, antecedents • Operant Conditioning • Focus on consequences of behaviours • Stimulus-Response (S-R) Models • Focus on stimulus-response connections - chains
Classical Conditioning • Pavlov US UR US UR CS CS CR U = unconditioned; C = conditioned S = stimulus; R = response
Classical Conditioning • 3 features of classical conditioning: • Extinction • Discrimination • Generalisation • Alarms
Operant Conditioning • Positive Reinforcement • Primary • Social • Secondary • Stimulatory • Rewards for appropriate toileting • Developing toileting skills • Dry pants training
Stimulus - Response • Toileting behaviour is made up of a series of stimulus-response connections – a chain • Problems: • Lack of training opportunity to establish chain • Decreased learning ability – less strength between links • CNS damage, weaker perception of stimuli • CNS damage resulting in reduced control of eliminatory responses
The S-R model • 3 primary components: • Stimulus of full bladder • Remaining dry • Continent passing of urine • S-R model underpins forward and backward chaining
Some treatment approaches: • Training for pre-requisite skills • Token Systems / Dry Pants training • Alarms • Biofeedback • Timed v Individualised • Intensive training
Pre-requisite skills • Assessment may indicate that the person lacks skills in finding the toilet, dressing / undressing, appropriate voiding, hygiene, etc • Following functional analysis these skills can be developed • Techniques could include task analysis, backward chaining, positive reinforcement, fading & generalisation
Dry Pants Training • Based on operant conditioning and token economy • Assumes that learner is physically able to achieve continence • Assumes that the “token” is reinforcer • “Whole day” may be too big a target • May focus on failures • Stress & anxiety may lead to failure • May inadvertently encourage punishment
Monday Tuesday Wed Thurs Friday Saturday Sunday Week 1 Week 2 Week 3 Week 4 Smiling Faces – awarded for “dry days” A recipe for failure?
Alarms • May be used in pants or in bed • Aim to pair sphincter contraction and waking with full bladder sensation • May be linked with “Dry Bed” or Dry Pants” training • Assumes learner has physical potential to achieve • Various problems reported with alarms, and their use in practice
Alarms & Classical Conditioning • Developed by Mowrer & Mowrer (1938) US UR micturition Bladder distension US UR Sphincter contraction / waking CS alarm CS CR Sphincter contraction / waking Bladder distension
Alarm interventions for nocturnal enuresis in children • Glazener & Evans (2002). 22 trials / 1125 subjects • Alarm interventions are an effective treatment for nocturnal bedwetting in children. • Desmopressin and tricyclics appeared as effective while on treatment, but this effect was not sustained after treatment stopped, • and alarms may be more effective in the long term. (see Prodigy guidelines)
Bladder Training • Involves the gradual postponing of voiding at first desire, and enforced voiding at set times, gradually prolonging interval, and hopefully bladder capacity • May use “overlearning” • Retention control training using shaping • Requires baseline measurement • May be implemented with pelvic floor muscle training, biofeedback & / or medication
Timed Waking in Nocturnal Enuresis • Best to use a “staggered” schedule to avoid limiting bladder capacity • Eg: 1hr, 3hr, 1.5 hrs, 4hrs • May cause voiding on approach, rather than waking • May be tiring or too difficult for carers to implement • Can be implemented with “overlearning”
Timed v Regular toileting • Timed toileting involves individualised toileting regimes to reflect usual frequencies • Regular toileting is a pre-determined schedule • Both approaches may have some value in preventing continence, though may also limit independence • Training effect may be more limited
Timed v Regular in elderly care • Southern & Henderson (1990) developed individualised timed schedules for 180 elderly hospital patients • Of the average of 8 toilet visits daily, only about 2 were successful • 1 week of baseline data was collected using pants alarms & / or checking, to identify “clusters” • Intervention greatly reduced unsuccessful toileting and incontinence episodes • They claimed in addition to save a great deal of nursing time that could be used on activities other than toileting
Systematic Reviews (Cochrane Database) • Prompted voiding for the management of urinary incontinence in adults: • 5 studies / 355 subjects, Eustice, Roe & Paterson (2000) • prompted voiding increased self-initiated voiding & decreased incontinent episodes in short-term…no evidence re: long-term effects. • A single small trial suggested that adding the muscle relaxant, Oxybutinin, reduced the number of incontinent episodes in the short-term • insufficient evidence to reach firm conclusions for practice
Biofeedback • Useful for urge or stress incontinence • May be based on feedback on detrusor pressure, or more general measures of relaxation through galvanic skin response (GSR) or electromyography (EMG) • Use of appropriate sensors illustrate effect of effort in contracting pelvic floor muscles
Biofeedback equipment with perineometer probes and LCD monitor Biofeedback session monitor output – patient has to follow the white line with pelvic floor contractions
Evaluation of Biofeedback • Burgio et al (1998) evaluated Biofeedback against Drug treatment and controls in a 6 year study of 197 women in a RCT • Biofeedback was significantly more effective, and was significantly more satisfactory to patients (however there are some limitations to the study)
Behavioural and cognitive interventions with or without other treatments for defaecation disorders in children - Brazzelli & Griffiths (2001) • A review of 16 randomised trials with a total of 843 • no evidence that biofeedback training adds any benefit to conventional treatment in the management of encopresis and constipation in children. • some evidence that behavioural intervention plus laxative therapy, rather than behavioural intervention or laxative therapy alone, improves continence in children with encopresis
Figure 3.-Proportions of subjects by group who reduced frequency of incontinence by 100%, 75%, and 50%. From: Burgio: JAMA, Volume 280(23).December 16, 1998.1995-2000
Intensive Training • A variation of Dry Pants • Developed by Azrin & Foxx (1971) • Claimed great success (in 4 hours!) • Involves intensive practice throughout the day, with increased fluids, positive reinforcement, and pants & toilet alarms • Very labour intensive • May be impractical at home • May pose ethical problems • See abstract here ゥ Richard Ingram / UWE Bristol 2001
Summary • There are a wide range of psychological models of continence, and associated treatments • Behavioural interventions are based on learning theories • They must be preceded by full assessment • Often they can be combined successfully with other approaches • Often they may achieve greatest success with fewer side-effects
References • Azrin, N. H., & Foxx, R. M. (1971). A rapid method of toilet training the institutionalized retarded. Journal of Applied Behavior Analysis, 4, 89-99 • Blackwell, C. (1989). A guide to the treatment of enuresis for professionals. Bristol: Enuresis Resource and Information Centre (ERIC). • Brazzelli M, Griffiths P. (2002). Behavioural and cognitive interventions with or without other treatments for defaecation disorders in children (Cochrane Review). In: The Cochrane Library, Issue 1, 2002. Oxford: Update Software. • Burgio KL, Locher JL. Goode PS. Hardin JM. McDowell BJ. Dombrowski M. Candib D. (1998). Behavioral vs. drug treatment for urge urinary incontinence in older women. A randomized controlled trial. JAMA December 16, 1998;280:1995-2000, • Butler, R.J. (1987). Nocturnal Enuresis: Psychological Perspectives. Bristol: Wright. • Butler, R.J. (1993). Enuresis Resource Pack: charts, questionnaires and information to assist professionals. Bristol: Enuresis Resource and Information Centre (ERIC). • Eustice S, Roe B, Paterson J. (2002). Prompted voiding for the management of urinary incontinence in adults (Cochrane Review). In: The Cochrane Library, Issue 1, 2002. Oxford: Update Software.
References • Getliffe, K., Dolman, M. (1997). (Editors). Promoting continence: A clinical and research resource. London: Bailliere Tindall. • Glazener CMA, Evans JHC. (2002). Alarm interventions for nocturnal enuresis in children (Cochrane Review). In: The Cochrane Library, Issue 1, 2002. Oxford: Update Software. • Lucas, M., Emery, S., & Beynon, J. (Editors) (1999). Incontinence. Oxford: Blackwell Science. • Morgan, R. (1984). Behavioural Treatments with Children. London: Heinemann • Morgan, R. (1993). Guidelines on minimum standards of practice in the treatment of enuresis. Bristol: Enuresis Resource and Information Centre (ERIC). • Resnick NM. (1998) Improving treatment of urinary incontinence [Editorial]. JAMA December 16,;280:2034-5.
References • Smith, P.S., & Smith, L.J. (1987). Continence and incontinence: Psychological approaches to development and treatment. London: Croom Helm. • Southern, D., & Henderson, P. (1990). Setting standards: tackling incontinence. Nursing Times, 86(10):36-8, Mar 7-13 • White, H. (1997). Incontinence in perspective. Chapter 1 IN Getliffe, K & Dolman, M (Editors). Promoting continence: A clinical and research resource. London: Bailliere Tindall. • Yule, W., & Carr, J. (1987). Behaviour modification for people with mental handicaps. London: Croom Helm.
Useful Links • Prodigy guidelines on nocturnal enuresis • http://www.prodigy.nhs.uk/guidance.asp?gt=Enuresis%20-%20nocturnal • EMG / biofeedback • http://www.veritymedical.co.uk/modes/EMG.htm • The Continence Foundation • http://www.continence-foundation.org.uk/ • Writing a project • http://www.continence-foundation.org.uk/in-depth/project-work-in-continence-care.php • ERIC • http://www.eric.org.uk/ • CINAHL Search • http://dialspace.dial.pipex.com/town/nhspeople/d/adag86/student/files/continence.pdf