Download

1 / 51
510 likes | 627 Views
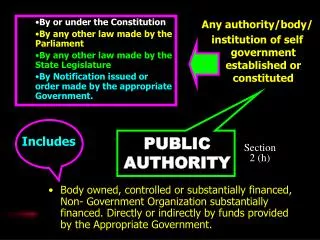
Public Authority meeting 26 July 2011. http://www.hta.gov.uk http://www.facebook.com/HumanTissueAuthority http://twitter.com/HTA_UK. Framework for living organ donation assessment. 26 July 2011 Allan Marriott-Smith. Background.

E N D
Public Authority meeting26 July 2011 http://www.hta.gov.uk http://www.facebook.com/HumanTissueAuthority http://twitter.com/HTA_UK
Framework for living organ donation assessment 26 July 2011 Allan Marriott-Smith
Background November 2010 - Authority agreed more work required on assessing living donation cases where risk of reward was considered greater. January to May 2011 - Further exploratory work on the issues at stake. June 2011 - Policy Members’ Group sketched out a solution.
Living kidney donation in the Netherlands Emma K. Massey, PhD Kidney Transplant Unit Erasmus MC, Rotterdam, the Netherlands
Alternative living donor programmes in R’dam • National paired exchange programme since 2004 (Exchange donors) • In Rotterdam, an altruistic donor programme since 2000: • Non-directed to the waiting list • Directed • Domino-paired
Domino-paired procedure Domino donor D Waiting List 1. 2. 3. 4. Altruistic donor R Paired-exchange couple
Screening in Rotterdam All living donors • Medical screening by nephrologist and other specialists • Psychosocial screening by a Transplant Coordinator • Understanding of risks • Motivation • Coercion • Consultation with the social worker • Financial and work considerations Altruistic donors (no genetic or emotional relationship) • A consultation with a psychologist (in addition to the steps above) • On indication
Altruistic donation Rotterdam 2000-2010 187 80 73 donated • 39 decided not to donate • rejected anonymity • 2 medical problems 8 still thinking 15 referred 122 • still in screening • 1 referred 11 medical problems 10 psychological problems 9 decided not to donate 4 decided not to donate 3 scheduled
Altruistic donation rotterdam 2000-2010 DONATED TRANSPLANTS Directed (non anonymous) 10 10 Waiting list 19 19 Domino Paired 44 96 Total 73 125
Conclusions • Genetically unrelated donors now outstrips genetically related donors • Donation via alternative programmes now makes up 30% of the total donor population • Paired-exchange donors • Altruistic donors • Directed altruistic donation is not common
Thank you!Questions? e.massey@erasmusmc.nl
Public Authority meeting26 July 2011 http://www.hta.gov.uk http://www.facebook.com/HumanTissueAuthority http://twitter.com/HTA_UK
Framework for living organ donation assessment 26 July 2011 Allan Marriott-Smith
Living Donation Assessment Process – As Is PESTEL – major external drivers for change that may have an impact on the HTA over the next five years Political eg change of government Economic eg impact of recession Sociological eg lifestyle changes affect transplant needs Technological eg smarter IT changes communication Environmental eg flu pandemic Legal eg new European legislation
Public Authority meeting26 July 2011 http://www.hta.gov.uk http://www.facebook.com/HumanTissueAuthority http://twitter.com/HTA_UK
Review of the Year26 July 2011 http://www.hta.gov.uk http://www.facebook.com/HumanTissueAuthority http://twitter.com/HTA_UK
Review of the Year 2011: The HTA Approach to Regulation 26 July 2011 Alan Clamp
Overview • Effective regulation – getting the balance right • Principles of better regulation – how do we measure up? • What next – meeting the challenges and making the most of the opportunities • Questions
Getting the balance right • More regulation – higher standards; increased public confidence; burden on establishments; increased costs • Less regulation – reduced burden; decreased costs; greater variability in standards; decreased public confidence • Focused regulation – proportionate, targeted and based on risk; maximising efficiency and effectiveness
How do we measure up? Proportionate, targeted and consistent: • the starting point is advice and guidance • regulatory action is based on risk (compliance and activity-based) and impact (immediate and indirect) • sliding scale (depending on risk and impact) with variable pace of escalation
How do we measure up? Transparent and accountable: • objective approach - clear decision-making processes based on robust evidence and sector expertise • monitored – published inspection reports, tracking shortfalls to ensure they are addressed, quarterly Regulatory Activity Reports and Annual Summary Compliance Report
What next? • Further development of risk-based and proportionate regulation • Improving the design of new regulations and how they are communicated (EUODD) • Greater collaboration with other regulators to share information, produce joint guidance, and maximise opportunities for joint and proxy inspection activity • Simplifying and modernising existing regulations
Review of the Year26 July 2011 http://www.hta.gov.uk http://www.facebook.com/HumanTissueAuthority http://twitter.com/HTA_UK
Context for today’s debate 26 July 2011 Victoria Marshment
Background • First living organ donation in 1954 between twin brothers • In the UK there are programmes for living kidney and liver (lobe) donation • Donation between family members or friends • Regulated by the HTA to ensure that there is no reward involved and that the donor is not being pressured –freely given consent • 150 Independent Assessors based across the UK • 1200 cases approved by the HTA in 2010/11
Why the debate? • Range of enquiries on relationships in living organ donation • More distant relationships including friends of friends, friends of family members and people who have met online • Our experience tells us that pressure can often be intense within families • A genetic relationship does not always mean that the two people involved really know each other
Next steps • The debate today will form part of our engagement on the assessment of living organ donations • We will use the information to aid the development of a risk based system • Continue to provide a robust, proportionate and transparent system
www.hta.gov.uk http://twitter.com/HTA_UK http://www.Facebook.com/HumanTissueAuthority
Review of the Year26 July 2011 http://www.hta.gov.uk http://www.facebook.com/HumanTissueAuthority http://twitter.com/HTA_UK
Questions • There are now more ways in which people can form relationships, including online routes. Do you think this has the potential to increase the numbers of living organ donors? Yes/No • Do you think there is more or less risk for such donors to be pressurised to give organs, compared with those donating to their family members? More/Less • Do you think there is more or less risk of reward or money changing hands in remote relationships, compared with donation between family members? More/Less • Would you be more likely to donate to an identified person rather than someone not identified and whom you may never know? Yes/No
Review of the Year26 July 2011 http://www.hta.gov.uk http://www.facebook.com/HumanTissueAuthority http://twitter.com/HTA_UK
Living kidney donation in the Netherlands Emma K. Massey, PhD Kidney Transplant Unit Erasmus MC, Rotterdam, the Netherlands
Altruistic donation rotterdam 2000-2010 DONATED TRANSPLANTS Directed (non anonymous) 10 10 Waiting list 19 19 Domino Paired 44 96 Total 73 125
Case study 1 • A dialysis patient became faint whilst waiting for her child in the school playground • Another mother came to her assistance and enquired as to the problem • After some consideration the mother decided to donate her kidney Patient-Donor had: • no previous relationship • were acquainted with one another, affinity as mothers, to the school • motivation to help • donation was approved
Are rewards less likely in living-related donation? (#39) • Study among 250 living donors • Spontaneous reports of ‘gifts’ from the recipient ranging from… ” (van Buren et al 2010)
Is risk of rewards higher when there is no emotional bond with the recipient? (#40) • Affinity (bond) can be to the (patient) group as a whole rather than a specific individual • Research among altruistic donors: • Experience with kidney disease in direct environment (50%) • Experience with chronic disease in direct environment (33%) • Death of a loved one (29%) • Donation and altruism as a way of life (71%) (Massey et al 2010)
What are our safeguards to prevent reward? Our system is based on: • Altruism • Autonomy • Freedom of choice • Assessed on a case-by-case basis • Final decision lies with the doctors in the transplant team
Conclusion Donors with ‘remote relationships’ are not common in the Netherlands The relationship does not necessarily determine the level of risk Financial rewards can occur in both living related and unrelated donation Altruistic motives are common among donors with no emotional or genetic relationship with the recipient If questioned the likelihood of a socially desirable answer is very high There is no watertight system to prevent financial rewards
References • van Buren et al (2010). For Love or Money? Attitudes Toward Financial Incentives Among Actual Living Kidney Donors. American Journal of Transplantation, 10, 2488-92. • Massey et al (2010). Encouraging Psychological Outcomes After Altruistic • Donation to a Stranger. American Journal of Transplantation, 10, 1-8. • Massey et al (2011). In Weimar, Bos & Busschbach. Organ Transplantation: Ethical, Legal and Psychosocial Aspects. Expanding the European Platform.
Thank you!Questions? e.massey@erasmusmc.nl
An altriustic donor “My mother got ill suddenly and her kidneys weren’t working anymore. She went on dialysis twice but decided that she didn’t want that. Two weeks later she had died. I offered her my kidney but she was too ill. After reading an article in the newspaper, I decided to donate my kidney to a stranger in the hope that that person would benefit from it for a long time. I did it with love!” (Massey et al. 2011)