Download
1 / 32
400 likes | 1.17k Views
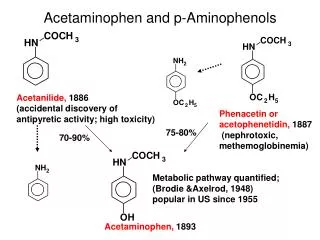
ACETAMINOPHEN. Active metabolite of phenacetin Weak COX-I and COX-2 inhibitor No significant anti-inflammatory effects Pharmacokinetics: Peak blood level is reached in 30-60 min Metabolized by hepatic microsomal enzymes and form acetaminophen sulfate and glucronide

E N D
ACETAMINOPHEN • Active metabolite of phenacetin • Weak COX-I and COX-2 inhibitor • No significant anti-inflammatory effects Pharmacokinetics: • Peak blood level is reached in 30-60 min • Metabolized by hepatic microsomal enzymes and form acetaminophen sulfate and glucronide • N-acetyl-p-benzo-quinoneimine (NAPQI)-Toxic to liver and kidneys
Indications • 325 – 1000mg (total dose not > 4000mg) • Headache, myalgia, postpartum pain • In rheumatoid arthritis with anti-inflammatory agent • Preferred to aspirin in peptic ulcer, in children with viral infections
Adverse effects • Mild increase in hepatic enzymes • Dizziness, excitement & disorientation at larger doses • Dose greater than 4-6 g/d is not recommended - cause liver damage • 15-20gm potentially fatal (30tablets)
Mechanism of hepatotoxicity of acetaminophen • NAP reacts with sulfhydryl gps in GSH normally & then excreted as mercapturic acid in urine but in toxic dose GSH is depleted and toxic metabolite accumulates Treatment • Supportive therapy • N-Acetylcysteine
COX-2 SELECTIVE INHIBITORS • Celecoxib, rofecoxib, valdecoxib, parecoxib, etoricoxib, lumaricixib • Inhibit prostaglandin synthesis by the COX-2 isozyme • Analgesic, antipyretic and anti inflammatory effects • No effect on platelet aggregation • No cardioprotective effect
CELECOXIB • Highly selective COX- 2 inhibitor. • Half life is 11 hrs • Metabolized mainly in the liver • Effective in rheumatoid arthritis and osteoarthritis. • Less production of peptic ulcer • Inhibit COX 2 mediated prostacyclin synthesis in vascular endothelium- platelet aggregation
orSAARDs Slow acting anti-rheumatic drugs
RHEUMATOID ARTHRITIS • An immunologic disease • Synovial inflammation leading to cartilage damage and bone erosions and subsequent changes in joint integrity is the hallmark of the disease • Persistent, symmetrical peripheral arthropathy • Presentation: swollen, painful, stiff hands & feet • Treatments that arrest 0r slow progression by modifying disease itself
Mechanism of Action of DMARDs • diverse group of drugs with different & poorly understood mechanisms of actions • slow the bone damage associated with RA & affect more basic inflammatory mechanism than the NSAIDs • effects of DMARDs may take 6 wks to 6 months to become evident
DRUGS Non-biologic DMARDs Biologic DMARDs • Methotrexate • Azathioprine • Cyclophosphamide • Chloroquine & hydroxychloroquine • Cyclosporine • Leflunomide • Mycophenolatemofetil • Sulfasalazine • D-Penicillamine • Gold Salts • Abatacept • Rituximab • Tocilizumab • TNF-α blocking drugs • Adalimumab • Etanercep • Infliximab • Immunoabsorption apheresis
METHOTREXATE • First DMARD of choice • Used at much lower doses than those needed in cancer chemotherapy MOA At lower doses it inhibits aminoimidazole-carboxamide ribonucleotide (AICAR-inhibits AMP deaminase) transformylase & thymidylate synthetase that accounts for the suppression of the immunologic mechanisms underlying rheumatoid arthritis
Pharmacokinetics • 70% absorbed after oral administration • Metabolized to less active metabolite • Excreted principally in the urine, but upto 30% may be excreted in bile • Concentration may increase in presence of hydrochloroquine-reduces clearance or tubular secretion Other Clinical uses (15-25mg weekly) • juvenile chronic arthritis • psoriatic arthritis
Adverse effects • Nausea • Mucosal ulcers • Leukopenia, alopecia, stomatitis, GI ulceration • Progressive dose-related hepatotoxicity Contraindications • Pregnancy
AZATHIOPRINE • Synthetic DMARD MOA • Acts through metabolite 6-thioguanine • Suppresses inosinic acid (IMP) synthesis, B & T-cell function, IL-2 secretion & immunoglobin production • Production of 6-thioguanine is dependent on thiopurinemethyltransferase (TMPT)
Adverse effects • Bone marrow suppression • GI disturbances • Infection risk • Lymphoma • Allergic rash & hepatotoxicity rarely
CYCLOPHOSPHAMIDE • Synthetic DMARD • Major metabolite phosphoramide mustard cross links DNA to prevent cell replication MOA • Suppresses T cell & B cell function by 30-40% • T cell suppression is responsible for clinical response in RA
Adverse effects • Dose related infertility in both sexes • Bone marrow suppression • Alopecia, hemorrhagic cystitis DOSE: orally 2mg/kg/d RA, SLE, vasculitis
CHLOROQUINE & hydroxychloroquine • Supress T-lymphocyte responses to mitogens • Decreased leukocyte chemotaxis • Stabilizing of lysosomal enzymes • Inhibition of DNA & RNA synyhesis • Trapping of free radical DOSE: 200mg/d
CYCLOSPORINE • A peptide antibiotic • Non-biologic DMARD • Inhibits IL-1 & 2 production through gene regulation • Inhibiting macrophage-T cell interaction • Metabolized by CYP3A4 • Leukopenia, thrombocytopenia • Cardiac toxicity, bladder cancer • Sterility
LEFLUNOMIDE • Nonbiologic DMARD • Inhibits T-cell proliferation by inhibiting RNA synthesis (pyrimidine synthesis) • Inhibits T-cell proliferation & production of autoantibodies by B-cells • Inhibits bony damage • As effective as methotrexate • Diarrhea (25% pts) • Mild alopecia, weight gain & increased BP
SULFASALAZINE • Metabolized to sulfapyridine & 5-aminosalicylic acid • IgA & IgM RF reduced • Supression of T-cell response & inhibition of B-cell proliferation • Inhibits release of inflammatory cytokines • Reduces radiologic disease progression • Nausea, vomiting, headache, rash • Neutropenia, hemolytic anemia, methhemoglobinemia, pulmonary toxicity
GOLD MOA • alters the morphology & functional capabilities of human macrophages I/M formulations: aurothiomalate & aurothioglucose Oral formulations: auranofin
Adverse effects • pruritic skin rashes with eosinphilia • stomatitis, metallic taste • hematologic abnormalities • proteinuria , nephrotic syndrome
RITUXIMAB • Biologic DMARD-Chimeric monoclonal antibody • Targets B lymphocyte through cytotoxicity & apoptosis • Depletion of B lymphocytes decreases inflammation by decreasing presentation of antigens to T lymphocytes & inhibiting secretion of proinflammatory cytokines • IV infusions 1000mg 2 weeks apart repeated 6-9 mths • Infusion reactions (pretreatment with glucocorticoids)
ABATACEPT • Biologic DMARD-T-cell costimulation blocker • Inhibits activation of T-cells • Monthly infusion after induction at 0, 2 & 4 wk • Reduces clinical signs & symptoms of RA including slowing of radiographic progression • Slightly increased risk of infections (should not be used in combination with TNF-a antagonists) • Possible increase in lymphomas
TNF-α blocking drugs • Biologic DMARDs • Anti-TNF antibodies inhibit T cell & macrophage function, & subsequently interfering with TNF-α • Adalimumab • Infliximab • Etanercept
Adverse effects • Increased risk of bacterial infections • Opportunistic infections • Increased risk of macrophage-dependent infections (TB)- screening of latent or active TB • Lymphoma risk