Download
1 / 16
160 likes | 280 Views
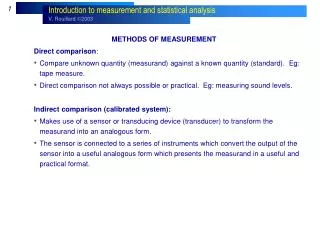
Theoretical Integration Using Methods of Template Comparison. Janice L. Penrod, PhD, RN, FGSA, FAAN Brenda L. Baney, MS Gwen E. McGhan, MN. Funding. The projects described were supported by:

E N D
Theoretical Integration Using Methods of Template Comparison Janice L. Penrod, PhD, RN, FGSA, FAAN Brenda L. Baney, MS Gwen E. McGhan, MN
Funding The projects described were supported by: NIH/NINR 1 R01NR010127; Exploring the Formal/Informal Caregiver Interface across 3 Death Trajectories PI: J. Penrod (2008-2012) NIH/NINR RO3 NR008538 Living with Uncertainty: Caregiving at the End of Life; PI: J. Penrod (2003-2005) The contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH/NINR
Aim The purpose of this study was to refine the final phase of the Model of Caregiving through the End of Life entitled “Reinventing Normal”
Model of End-of-life Caregiving Acknowledging the End of Life Confirming Suspicions Losing Normal Building a New Normal Reinventing Normal Sensing a Disruption Challenging Normal Certainty of Death Seeking Normal through Cognitive Restructuring Penrod, Hupcey, Shipley, Loeb, & Baney, 2011
Qualitative Research • Focus: concept or phenomenon of interest • Validity (or trustworthiness): • Descriptive • Interpretive • Theoretical • Conceptual co-occurrence: in reality concepts do not exist in isolation of one another • Therefore conceptual co-occurrence in the phenomenon of interest may be refined through a study of interrelationship among concepts manifest in a common phenomenon of interest
Theoretical Integration Using Techniques of Template Comparison • Exploration of the affiliation among related concepts in theoretical formulations of the phenomenon • Type of triangulation focused on refining theory—theoretical integration • Provides insights into further exploration of a concept and/or developing theory Morse & Penrod, 1999 Hupcey & Penrod, 2003
Method • Two theories describing the phenomenon of bereavement were integrated using template comparison • Theory 1: Bereavement: Reinventing Normal • Theory 2: Bereavement: The Other Side of Sadness (G. A. Bonnano, 2009)
Model of End-of-life Caregiving Acknowledging the End of Life Confirming Suspicions Losing Normal Reinventing Normal Sensing a Disruption Challenging Normal Building a New Normal Penrod, Hupcey, Shipley, Loeb, & Baney, 2011
Theory 1: BereavementReinventing Normal • Restructuring one’s life after death is a cyclical, reiterative process • Existential and situational uncertainties arise--sporadic • Pre-cognitive/cognitive insights are integrated through a process of reading the situation • Responsive strategies are enacted to manage these distressed states • Reformulated patterns of everyday life are assimilated • However, the reinvented normal is marked permanently by the loss and replete with memories Penrod, Hupcey, Shipley, Loeb, & Baney, 2011
Theory 1: BereavementReinventing Normal • Death described in detail; expressed understanding of illness and some degree of comfort with pain/symptom control • Experience described as a “roller coaster” as perspectives of past, present and future collide • Loss of caregiving routine disruptive; conscious effort to establish new routines in everyday life • Expressed sense of loneliness (dominant) and sadness (“for him or for me?”) • Overall, felt well supported by family, friends and others
Theory 1: BereavementReinventing Normal • “Can do” attitude prevailed—caregivers compared themselves to others who lived through a profound loss • Focused on “keeping busy” – from catching up on neglected household chores to post death finances to beginning new activities for personal health/enjoyment • Plans become more important—making lists; “unbearable if I wake-up without a plan” • Need to dispense of equipment/supplies related to illness difficult, but donations gave a sense of helping others during difficult times • Persistent disturbances in sleep pattern most commonly reported
Theory 1: BereavementReinventing Normal The negative case: • Expressed understanding of illness and some degree of comfort with pain/symptom control: Unrelenting suffering • Experience described as a “roller coaster” : dwelling on the death, unable to conceive any options for the future • Loss of caregiving routine disruptive; conscious effort to establish new routines in everyday life: energy invested the loss • Expressed sense of loneliness (dominant) and sadness (“for him or for me?”): overwhelming, incapacitating • Overall, felt well supported by family, friends and others: despite supportive network, does not feel connected • “Can do” attitude prevailed—caregivers compared themselves to others who lived through a profound loss: “can’t do” even what others have done • Focused on “keeping busy”: sleeping frequently; does “absolutely nothing”; smoking is “the only joy I got left” • Plans become more important: unable to formulate plans for the day or the future • Need to dispense of equipment/supplies related to illness difficult; “hospice came, they cleaned up the pills and everything that was here and got rid of them”
Theory 2: BereavementThe Other Side of Sadness • Initially, present focused - “Whatever it takes to get through the night” • Humans have a capacity to thrive in the face of adversity – we are hardwired to deal with loss, “resilience” • Recalibrate to the reality of the loss through adaptive oscillation between sadness (inward reflection) and more positive emotions such as laughter or reminiscing which reconnects us with those around us (outward expression) • This oscillation over time widens in cycle and there is a return to a state of equilibrium • Enduring bond with the deceased • Individualized and highly reflective of culture – grief does not unfold in a five-stage process Bonnano, 2009
Theory 2: BereavementThe Other Side of Sadness • Not everyone copes well with loss • Coping Flexibility – resilient people have more tools in their toolbox: • Ability to switch from sadness to positive emotions • More flexible in the way they use emotions • Behavioral Flexibility – cope by using behaviors or strategies that under normal circumstances are less than perfectly healthy • Blame external factors • Self-serving biases • Genetic component and psychological factors are involved Bonnano, 2009
Results • Significant conceptual congruence between the two theories • Areas for further exploration: • The concept of resilience appears to be significant to understanding supportive care for caregivers • Coping flexibility was reflected in the EOL caregiving study, not only in bereavement but also in earlier phases of caregiving
Conclusions • This template comparison verified the primary theoretical assertions in the bereavement phase of The Model of Caregiving through the End of Life and exposed promising avenues for further investigation • Nurses are pivotal in supporting family caregivers across illness trajectories and through bereavement • Supportive care begins with nurses’ awareness of the phenomenon and will be extended through theoretical refinement that guides theory-based, evidence-driven practice