Download

1 / 26
260 likes | 453 Views
|. Dehydration Paul R. Earl Facultad de Ciencias Biológicas Universidad Autónoma de Nuevo León San Nicolás, N. L., Mexico pearl@dsi.uanl.mx.

E N D
| Dehydration Paul R. Earl Facultad de Ciencias Biológicas Universidad Autónoma de Nuevo León San Nicolás, N. L., Mexico pearl@dsi.uanl.mx
Dehydrationorvolumedepletionisclassifiedasmild, moderateorseverebasedonhowmuchbodyfluidislost. Whensevere, dehydrationisalife-threateningemergency.Volume depletion denotes lessening of the total intravascular plasma, whereas dehydration denotes loss of plasma-free water disproportionate to the loss of sodium. Potassium and other electrolytes including buffers líke phosphates need to be considered. Children, especially those younger than 4 years old, are more susceptible to volume depletion as a result of vomiting, diarrhea or increases in insensible water losses.
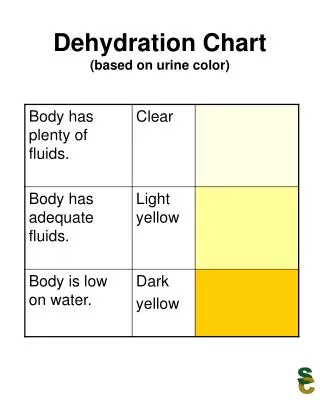
Dehydrationcanbecausedbylosingtoomuchfluid, notdrinkingenoughwaterorfluids, orboth. Vomitinganddiarrheaarecommoncauses. • Dehydrationisclassifiedasmild, moderateorseverebasedonhowmuchbody'sfluidislost. Symtonsinclude: • Dryorstickymouth. • Dizziness. • Lowornourineoutput; concentratedurineisdarkyellow. • Notproducingtears. • Sunkeneyes. • Markedlysunkenfontanelles (thesoftspotonthetopoftheheadinababy). • Lethargicorcomatose.
Inadditiontothesymptomsofactualdehydration, youmayalsohave: • vomitingand • diarrhea. • Drinkingfluidsisusuallysufficientformilddehydration. Itisbettertohavefrequent, smallamountsoffluid (usingateaspoonorsyringeforaninfantorchild) ratherthantryingtoforcelargeamountsoffluidatonetime. Drinkingtoomuchfluidatoncecanbringonmorevomiting. • Electrolytesolutionsorfreezerpopsareespeciallyeffective. Theseareavailableatpharmacies. Sportdrinkscontainalotofsugarandcancauseorworsendiarrhea. Ininfantsandchildren, avoidusingwaterastheprimaryreplacementfluid.
Intravenousfluidsandhospitalizationmaybenecessaryformoderatetoseveredehydration. Thedoctorwilltrytoidentifyandthentreatthecauseofthedehydration. • Treatmentincludesstarting NS@20ml/kgslowpushuntilsignsofseveredehydrationdisappear. AvoidRingerLactatetillpatientpassesurine. Maintainencefluiddependsonbodyweight. Either DNS or RL maybeused 10kg andless 100ml/Kg 10-20 Kg 1000mL+50ml/kg 20+ Kg 1500ml+ 20 ml/kgItmaybeadvisabletogivehalfthecalculatedfluidinthefirst 8 hoursandtheremainingoverthenext 16 hours • Precautions • checkforpulmonaryoedemareplenishPotassiumasrequiredChillsmayoccurduetofluidadministrationruleoutinfectiouscauses
Most cases of stomach viruses (also called viral gastroenteritis) tend to resolve on their own after a few days. • Boxers under hot lights sip water, then usually spit it out. They don`t seem to know that that water could save them from a coma during heat prostration! • Pathophysiology • Pediatric dehydration is frequently the result of gastroenteritis, characterized by vomiting and diarrhea. However, other causes of dehydration may include poor oral intake due to diseases such as stomatitis, insensible losses due to fever, or osmotic diuresis from uncontrolled diabetes mellitus.
Pathophysiology • Pediatric dehydration is frequently the result of gastroenteritis, characterized by vomiting and diarrhea. However, other causes of dehydration may include poor oral intake due to diseases such as stomatitis, insensible losses due to fever, or osmotic diuresis from uncontrolled diabetes mellitus. • Volume depletion denotes lessening of the total intravascular plasma, whereas dehydration denotes loss of plasma-free water disproportionate to the loss of sodium. The distinction is important because volume depletion can exist with or without dehydration, and dehydration can exist with or without volume depletion
In children with dehydration, the most common underlying problem actually is volume depletion, not dehydration. Intravascular sodium levels are within the reference range, indicating that excess free water is not being lost from plasma. Rather, the entire plasma pool is contracted with solutes (mostly sodium) and solvents (mostly water) lost in proportionate quantities. This is volume depletion without dehydration. The most common cause is excessive extrinsic loss of fluids.
Pediatric patients, especially those younger than 4 years, tend to be more susceptible to volume depletion as a result of vomiting, diarrhea, or increases in insensible water losses. Significant fluid losses may occur rapidly. The turnover of fluids and solute in infants and young children can be as much as 3 times that of adults. This is because of the following: • Higher metabolic rates • Increased body surface area to mass index • Higher body water contents (Water comprises approximately 70% of body weight in infants, 65% in children, and 60% in adults.)
Sodium considerations • Volume depletion can be concurrent with hyponatremia. This is characterized by plasma volume contraction with free water excess. An example is a child with diarrhea who has been given tap water to replete diarrheal losses. Free water is replenished, but sodium and other solutes are not.
In hyponatremic volume depletion, the person may appear more ill clinically than fluid losses indicate. The degree of volume depletion may be clinically overestimated. Serum sodium levels less than 120 mEq/L may result in seizures. If intravascular free water excess is not corrected during volume replenishment, the shift of free water to the intracellular fluid compartment may cause cerebral edema.With true dehydration, plasma volume contracts with disproportionate further free water loss. An example is the child with diarrhea whose fluid losses have been replenished with hypertonic soup, boiled milk, baking soda, or improperly diluted infant formula. Volume has been restored, but free water has not.
In hypernatremic volume depletion, the patient may appear less ill clinically than fluid losses indicate. The degree of volume depletion may be underestimated. Usually, at least a 10% volume deficit exists with hypernatremic volume depletion.As in hyponatremia, hypernatremic volume depletion may result in serious central nervous system (CNS) effects as a result of structural changes in central neurons. However, cerebral shrinkage occurs instead of cerebral edema. This may result in intracerebral hemorrhage, seizures, coma, and death. For this reason, volume restoration must be performed gradually over 24 hours or more. Gradual restoration prevents a rapid shift of fluid across the blood-brain barrier and into the intracellular fluid compartment.
Potassium considerations • Potassium shifts between intracellular and extracellular fluid compartments occur more slowly than free water shifts. Serum potassium level may not reflect intracellular potassium levels. Although a potassium deficit is present in all patients with volume depletion, it is not usually clinically significant. However, failure to correct for a potassium deficit during volume repletion may result in clinically significant hypokalemia. Potassium should not be added to replacement fluids until adequate urine output is obtained.
Acid and base problems • Clinicians may observe derangements of acid-base balance with volume depletion. Some degree of metabolic acidosis is common, especially in infants.Mechanisms include bicarbonate loss in stool and ketone production. Hypovolemia causes decreased tissue perfusion and increased lactic acid production. Decreased renal perfusion causes decreased glomerular filtration rate, which, in turn, leads to decreased hydrogen (H+) ion excretion. These factors combine to produce a metabolic acidosis.
In most patients, acidosis is mild and easily corrected with volume restoration (as increased renal perfusion permits excretion of excess H+ ions in the urine). Administration of glucose-containing fluids further decreases ketone production. Frequency United States Pediatric dehydration, particularly that due to gastroenteritis, is a common ED complaint. Approximately 200,000 hospitalizations and 300 deaths per year are attributed to gastroenteritis each year.
International According to the Centers for Disease Control and Prevention (CDC), for children younger than 5 years, the annual incidence of diarrheal illness is approximately 1.5 billion, while deaths are estimated between 1.5 and 2.5 million. Though these numbers are staggering, they actually represent an improvement from the early 1980s, when the death rate was approximately 5 million per year.
Mortality/Morbidity • Morbidity varies with the degree of volume depletion and the underlying cause. • The severely volume-depleted infant or child is at risk for death from cardiovascular collapse. • Hyponatremia resulting from replacement of free water alone may cause seizures. • Improper management of volume repletion may cause iatrogenic morbidity or mortality.
Age • Infants and younger children are more susceptible to volume depletion than older children. Clinical History The goal of the history and physical examination is to determine the severity of the child's condition. Classifying the degree of dehydration as mild, moderate, or severe accurately allows for appropriate therapy and disposition of the patient in a timely fashion. Obtaining a complete history from the parent or caregiver is important because it provides clues to the type of dehydration present.
The emergency physician should be diligent in obtaining the following information: • Feedingpattern and fluidsgiven • Number of wet diapers compared with normal • Fluid loss (eg, vomiting, oliguria or anuria, diarrhea) • Possibleingestions • Activity • Medications • Heat and sunlightexposures
Physical • The following table highlights the physical findings seen with different levels of pediatric dehydration.
Of these, the most accurate in identifying the level of dehydration are capillary refill, skin turgor, and breathing. The least accurate are mental status, heart rate and fontanelle appearance.
Causes • In most cases, volume depletion in children is from fluid losses from vomiting or diarrhea. • Vomiting may be caused by any of the following systems or processes: • CNS (eg, infections, space-occupyinglesions) • GI (eg, gastroenteritis, obstruction, hepatitis, liver failure, appendicitis, peritonitis, intussusception, volvulus, pyloric stenosis, toxicity [ingestion, overdose, drug effects]) • Endocrine (eg, diabeticketoacidosis [DKA], congenital adrenal hypoplasia, Addisonian crisis) • Renal (eg, infection, pyelonephritis, renal failure, renal tubular acidosis) • Psychiatric (eg, psychogenic vomiting) - This is not seen in infants and is rare in children compared with adults.
Diarrhea may be caused by any of the following systems or processes: • GI (e.g., gastroenteritis, malabsorption, intussusception, irritable bowel, inflammatory bowel disease, short gut syndrome) • Endocrine (eg, thyrotoxicosis, congenital adrenal hypoplasia, Addisonian crisis, diabeticenteropathy) • Psychiatric (eg, anxiety)
Volume depletion not caused by vomiting or diarrhea may be divided into renal or extrarenal causes. • Renal causes include use of diuretics, renal tubular acidosis, and renal failure (eg, trauma, obstruction, salt-wasting nephritis). The effects of diabetes insipidus, hypothyroidism, and adrenal insufficiency also fall into this category. • Extrarenal causes include third-space extravasation of intravascular fluid (eg, pancreatitis, peritonitis, sepsis, heart failure); insensible losses from fever, sweating, burns, or pulmonary processes; poor oral intake; and hemorrhage.