Download

1 / 13
180 likes | 599 Views
ACOUSTIC NEUROMA. Dr. Sudeeep K.C. Acoustic neuroma is also known as vestibular schwanoma or VIIIth nerve tumour . INCIDENCE: Acoustic neuroma constitutes 80% of all cerebellopontine angle tumours and 10% of all brain tumours. PATHOLOGY :

E N D
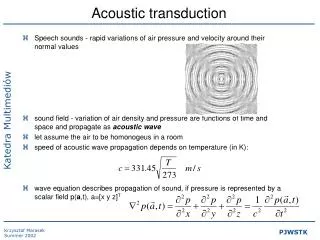
ACOUSTIC NEUROMA Dr. Sudeeep K.C.
Acoustic neuroma is also known as vestibular schwanoma or VIIIth nerve tumour. • INCIDENCE: Acoustic neuroma constitutes 80% of all cerebellopontine angle tumours and 10% of all brain tumours.
PATHOLOGY: • It is benign encapsulated, extremely slow growing tumour of viii th nerve. • Microscopically, it consists of elongated spindle cells with rod shaped nuclei lying in rows . Bilateral tumours are seen in patients with neurofibromatosis.
CLASSIFICATION • DEPENDING UPON THE SIZE, THE TUMOR IS CLASSIFIED:- • INTRACANALICULAR(CONFINED TO INTERNAL AUDITORY CANAL) • SMALL SIZE (UP TO 1.5 CM) • MEDIUM SIZE (1.5-4CM) • LARGE SIZE(> 4 CM)
CLINICAL FEATURES: 1) Age and sex: 40 to 60 yrs of age, both sexes are equally affected. 2)Cochleovestibular symptoms: It is the earliest symptoms when tumour is still intracanalicular. Progressive unilateral SNHL , often accompanied by tinnitus. Marked difficulty in understanding speech , out of propotion to the pure tone hearing loss .There is imbalance and unsteadiness.
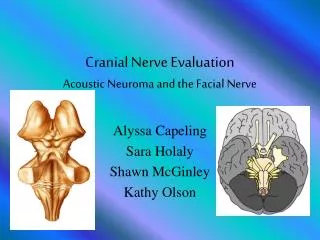
3)Cranial nerve involvement : • Vth nerve is the earliest to be involved Reduced corneal sensitivity, numbness or parasthesia of face. • VIIth nerve sensory fibres are affected early. • Hypoaesthesia of posterior meatal wall(Hitzelberger’s sign),loss of taste. Reduced lacrimation. • IXth and Xth nerves Hoarsness • Other cranial nerves affected when tumour is very large.
4) Brainstem involvement: Ataxia, weakness and numbness of arms legs with exaggerated tendon reflexes. • 5) Cerebellar involvement : Pressure symptoms on cerebellum are seen in large tumours. • 6)Raised intracranial tension : late feature, having headache, nausea, vomiting, diplopia ,papilloedema with blurring of vision.
INVESTIGATION • AUDIOLOGICAL TESTS • PURE TONE AUDIOMETRY SHOWS SNHL. • SPEECH AUDIOMETRY SHOWS POOR SPEECH DISCRIMINATION & DISPROPORTIONATE TO PURE TONE HEARING LOSS • RECRUITMENT PHENOMENON IS ABSENT. • SHORT INCREMENT SENSITIVITY INDEX (SISI) TEST WILL SHOW A SCORE OF 0-20% IN 70 –90% CASES • STAPEDIAL REFLEX DECAY TEST
VESTIBULAR TEST • CALORIC TEST WILL SHOW DIMINISHED OR ABSENT RESPONSE IN 96% OF PATIENTS.WHEN TUMOUR IS VERY SMALL,CALORIC TEST MAY BE NORMAL. • NEUROLOGICAL TESTS • COMPLETE CN FUNCTONS EXAMINATIO AND FUNDUS EXAMINATION • RADIOLOGICAL TESTS • PLAN X-RAY,CT-SCAN , MRI WITH GADOLINIUM CONTRAST, VERTEBRAL ANGIOGRAPHY.
ELECTRIC RESPONSE AUDIOMETRY • VERY USFUL TEST OF RETROCOCHLEAR LESION. • IN THE PRESENCE OF VIIITH NERVE TUMOUR, A DELAY OF>0.2MSEC IN WAVE V BETWEEN TWO EARS IS SIGNIFICANT . • CSF EXMINATION • PROTEIN LEVEL IS RAISED , LP IS AVOIDED .
TREATMENT: • Surgery: Surgical removal of tumour is the treatment of choice. • Radiation: Radiotherapy has no role in treatment of acoustic neuroma due to low tolerance of CNS to radiation. Gamma knife surgery for patient unfit for Surgery or who refuse surgery.