Download
1 / 50
500 likes | 668 Views
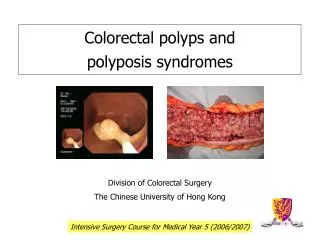
Polyposis Syndromes of the Colon Current Management, Controversies and Future Direction. Eric J. Dozois, MD Division of Colon & Rectal Surgery Mayo Clinic Rochester, Minnesota. Polyposis Schema. Inherited Polyposis Syndromes. Adenomatous Syndrome : Familial adenomatous polyposis

E N D
Polyposis Syndromes of the ColonCurrent Management, Controversies and Future Direction Eric J. Dozois, MD Division of Colon & Rectal Surgery Mayo Clinic Rochester, Minnesota
Inherited Polyposis Syndromes • Adenomatous Syndrome: • Familial adenomatous polyposis • mutY human homologue (MYH) • Hamartomatous Syndromes: • Peutz-Jeghers • Juvenile • Cowden’s • Ruvalcaba-Myhre-Smith
Non-Inherited Polyposis Syndromes • Cronkhite-Canada Syndrome • Hyperplastic Polyposis • Lipomatous Polyposis • Nodular Lymphoid Hyperplasia • Inflammatory Polyposis • Lymphomatous Polyposis
Polyposis Syndromes • Adenomas and hamartomas • Low incidence, Autosomal dominant • Colorectal Malignancies • Extra-colonic malignancies • Controversies in management • Need for Genetic Counseling
Inherited Polyposis Syndromes • Elucidation of underlying gene mutations • Understanding of cell biology and molecular mechanisms associated with cancer pathogenesis • Allows refined categorization, phenotype and cancer risk
Hamartomatous Syndromes CS PJS JP Incidence 1:200,000 1:120,000 1:100,000 Gene PTEN STK11 BMPR1A/SMAD4 Risk of CRC 10% Elevated 50% Extracolonic CA Yes Yes Yes
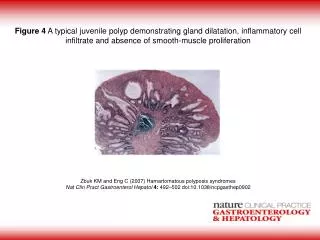
Juvenile Polyposis • Sporadic Juvenile polyps (2% Peds) • Hamartomas throughout GI tract • Rectal bleeding, anemia, intussusception • Capsule endoscopy is emerging tool for dx • *CRC risk 9% - 68%, mean age 34yrs • Extracolonic - Stomach, duodenal, • Genetic etiology in 50% remains elusive *Howe et al. Ann Surg Oncol 1998;5:751
JP – Surgical Management • Colectomy with IRA or IPAA: - Symptomatic bleeding - > 20 polyps - Dysplasia • Endoscopic Polypectomy: - < 20 polyps
Peutz-Jeghers Sydrome • 50-100 Hamartomas: - sb colon rectum stomach • Mucocutaneous melanin pigmentation
Peutz-Jeghers Syndrome • Hamartoma-adenoma-carcinoma sequence* • Intestinal & Extraintestinal cancers* • Ovarian sex-chord tumors, breast, pancreatic • Surgery – complications, malignancy *Wang et al. J Pathol 1999:188:9
PJS - Clinical Presentation • Abdominal cramping • Intussusception • Anemia
PJS - Management • Intussusception & Occult bleeding • Multiple laparotomies • Enteroscopy during laparotomy:* • Polyp clearance to reduce recurrent laparotomies • 4 of 25 patients required surgery in 14yrs *Phillips et al. Dis Colon Rectum 2003;46:48
Cowden Syndrome • Hamartomas of GI, skin, mucus membranes • Hallmark – facial trichilemmomas (wart-like) • GI CA risk – approx. 10% • Extra GI CA – *breast, *thyroid, GYN, retina • Surveillance and prevention of associated malignancies • Surgery for complications
Ruvalcaba-Myhre-Smith Syndrome • Described in 1980* • Gastrointestinal hamartomas • Macrocephaly, mental retardation, lipid storage myopathies, thyroiditis • Hyperpigmentation of penile skin • Alterations in PTEN gene • No CRC or extra-colonic cancer risk Ruvalcaba et al. Clin Genetics 1985;18:413
MYH-Associated Polyposis(mutY human homologue) • Base excision repair gene • Autosomal-recessive – family history • May account for the 7% - 8% of FAP phenotypes in whom no APC germ-line mutation has been identified* • Absence of strong multigenerational family history of polyposis • Difficult to distinguish from FAP, AFAP *Al-Tassen et al. Nat Genet 2002;30:227
MYH-Associated Polyposis(mutY human homologue) • Present between ages 45 – 60 yrs • Average number of adenomas = 16 (100s) • Carriers of bi-allelic and mono-allelic MYH mutations have a significantly increased risk of CRC* *Croitoru et al. J Natl Cancer Inst 2004;96:1631
Familial Adenomatous Polyposis • First reported in literature in 1841 • Autosomal dominant, APC mutation • 825 different germ-line mutations • Hundreds to thousands of polyps • 100% risk of colon cancer • Multiple extra-colonic manifestations
Familial Adenomatous Polyposis • Prophylactic Surgery • Timing of Surgery • Type of Surgery • Choice of Procedure • Choice of Technique
FAP – Type of Surgery • Colectomy with ileorectostomy • Proctocolectomy with IPAA • Anoproctocolectomy, ileostomy • Open or laparoscopic
FAP – Choice of Procedure • Cancer Prophylaxis • Technical feasibility • Complications • Functional Outcome - QOL
Management Controversy Ileal Pouch-Anal Anastomosis vs. Ileo-Rectostomy
Quality of Life after IPAA & IRAFamilial Polyposis • Time: 1981 - 1998 • IPAA (152 pts), IRA (32 pts) • No Difference in: • Early and late complications • Functional Results Hassan et al. Dis Colon Rectum 2005;48:2032
Comparison of SF-36 Physical and Mental Health Summary Scores p = 0.4 Physical Health Mental Health*
Functional Outcome after IRA Institution N Mean # BMs Continence QOL (24 hrs) Day/Night Cleveland 51 4 82/NA 93 Mayo 21 4 83/89 NA St. Marks 62 3 72/NA NA St. Antoine 23 3 98/96 NA Toronto 60 6 90/87 80
Functional Outcome after IPAA Institution N Mean # BMs Continence QOL (24 hrs) Day/Night Cleveland 62 5 75/74 95 Mayo 187 4 84/80 98 St. Marks 37 5 60/NA NA St. Antoine 171 4 98/96 NA Toronto 50 6 75/51 93
Rectal Cancer Rates After IRA Study No. Pts F/U Rectal CA Rate (yrs) (%) Bulow 659 11 7 Bertario 200 7 24 De Cosse 294 25 13 Sarre 133 20 12 Jarvinen 100 20 25 Iwama 320 20 37
FAP - Rectal Cancer • Independent Risk Factors:* • Age at colectomy (>40 yrs) • Length of time after IRA (12%/20yrs) • Number of polyps (> 1000) • Length of distal remnant (ileal-sigmoid) • Presence of colorectal malignancy • Genotype *Bjork et al. Dis Colon Rectum 2000;43:1719
FAP - Poor Results From IRA • Limited surgical options • Treatment and follow-up not routinely performed in specialized centers • Poor understanding of genotype-phenoptype correlation • Inadequate surveillance programs • Focus on “ease” of operation and functional outcome
Rectal Cancer Rates After IRAFunction of Available Surgical Options Timeline No. Pts F/U Cancer Rate (yrs) (%) Pre-pouch era 62 15 13 (1950-1982) Pouch era 135 5 0 (1983-1990) Church et al. DCR 2003;46:1175-1181
Genotype–Phenotype Correlation • Cancer Risk & Severity of Polyposis1: • > 1000 polyps = high risk • < 1000 polyps = 50% less risk • Severity of Polyposis - APC Mutation2: • Codon 1309 - leads to severe disease • Codons 3,4 – attenuated FAP 1Debinski et al. Gastro 1996;110:1028 2Church. Semin Colon Rectum Surg 1998;9:49
Molecular Genetic Tests as a Guide to Surgical Management of Familial Adenomatous PolyposisVasen et al. Lancet 1996;348:433-35 “Might information on the location of the mutation be useful in determining the most appropriate surgical treatment?”
Molecular genetic tests as guide to surgical management of FAP • APC mutation beyond codon 1275 Rectal CA Risk after IRA Risk of Rectal Excision Vasen et al. Lancet 1996;348:433-35
Genotype and Phenotype Factors for Rectal Cancer After IRA • 1955 – 1997 • 371 patients had IRA • Median follow-up 81 mos. • Multivariate analysis: • Sex, Age • No. rectal polyps, Colon CA • APC mutation Bertario et al. Ann Surg 2000;231:538
Results – Risk of Rectal CA • 10 years 7.7% • 15 years 13.1% • 20 years 23.0% Bertario et al. Ann Surg 2000;231:538
Results – Risk of Rectal CA • Univariate Analysis: • Colon cancer at initial operation • More than 30 polyps in the rectum • Mutation between codon1250 – 1464 • Multivariate Analysis: • Colon CA • Codons 1250 - 1464 9-Fold Increase Risk of Rectal Cancer Bertario et al. Ann Surg 2000;231:538
Arguments No Longer ValidIRA over IPAA • Functional results significantly better • Quality of life significantly better • Surgical complications are higher • Surveillance prevents cancer • Cancer can be cured if occurs • Can always do IPAA if CA develops
Ileal Pouch Neoplasia • Lifetime risk of neoplasia unknown • Adenomas form in 35% - 57% • Risk of developing adenomas: 5yrs (7%) 10yrs (35%) 15yrs (75%) • 13 Cancers reported: • Mucosectomy in 8 pts • CRC, multiple polyps Parc et al. Ann Surg 2001;233:360 Groves et al. Dis Colon Rectum 2005;48:816
FAP – Indication for IPAA • Age at time of surgery > 40yrs • > 1000 colonic polyps • > 20 Rectal Polyps • CRC at time of surgery • APC mutation - codon1250-1450 • Unreliable surveillance
FAP – IRA Acceptable? • Less than 1000 polyps in colon • Less than 20 polyps in the rectum • Attenuated FAP • APC mutation before 1250 or after 1450
ConclusionsPolyposis Syndromes of the Colon • Represent a wide spectrum of rare diseases with predisposition for both CRC and extra-colonic disease • A clear understanding of the differences between them ensures accurate diagnosis and proper management • Advances in molecular genetics will continue to provide even more insight to guide treatment