Download
1 / 32
340 likes | 552 Views
Three-Stage Sampling Plan. Stage 1: Randomly selecting particular sites (venues) within strata Stage 2: Randomly selecting sessions (half-days of operation within sites Stage 3: Randomly selecting respondents within sessions at selected sites. Stage 1: Sampling Sites. Two strata

E N D
Three-Stage Sampling Plan • Stage 1: Randomly selecting particular sites (venues) within strata • Stage 2: Randomly selecting sessions (half-days of operation within sites • Stage 3: Randomly selecting respondents within sessions at selected sites
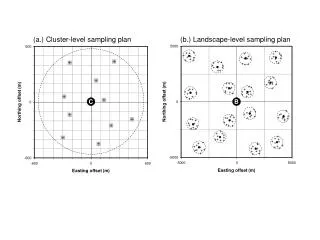
Stage 1: Sampling Sites • Two strata • STD clinics operated in L.A. County, Long Beach City (13 sites; 23,000 patients) • High-risk sexual environments • “Sites” are physical establishment (clinic) or physical entity (public park) • Locations that are co-located or proximal considered one “site” • Enumeration of sites in each stratum, with number of locations in each site
Stage 2: Sampling Scheduled Sessions • Each site sampled in Stage 1 will determine when MSM, MSM/W are most likely to congregate • Time blocks will be 4 hours (am, pm, eve) • Obtain reasonable estimate of how size is distributed across sessions • We will sample sessions with PPES • We will sample 90 sessions from each stratum (~ 7 sessions for STD sites; 4 sessions for sexual locations; Total sessions = 180
Stage 3: Sampling Participants within Scheduled Sessions • We will deploy 2 interviewers to each sampled session and location to target MSM and MSM/W for sampling and interviewing • Sample drawn sequentially
Branding and Visibility • High-profile study adopted by L.A. County and Long Beach City STD Programs • Press releases and information about the study through county materials • Announce study in gay magazines, local newspapers, websites • Flyers/postcards to local gay-oriented establishments • CAB to advise the study and visibility aspects
Index Participants: Screening Procedures • On specified sites and times, teams first capture number of MSM and MSM/W at location • Identify potential cohort member and explain this is a study of the sexual health of L.A./Long Beach area men and their sexual partners, both drug using and non-drug using • All cohort members will be asked to provide information about joining the study to at least 1 of their current sexual partners, especially female partners
Enrollment of Index Participants • Men screened will be given appointments at the field offices in Hollywood and Long Beach • Men who decline are thanked and visible information about the individual recorded • Consent procedures completed and data collection begins
Enrollment of Sexual Partners • Enrollment occurs indirectly • Materials describe the study and provide toll-free telephone number • Appointment is made from phone call • Partners asked to bring invitation materials to appointment for verification of the ask • Partners asked to provide consent for linking of data to index participant
Follow-up Assessments • Pre-paid calling cards provided to contact staff members • $50 compensation for self-report and biological samples (6- and 12-months) • Participants who terminate early will be asked to complete 5 to 10-minute discussions to solicit reasons for termination • Probes for positive and negative experiences
Interviewer Training • Approximately 50 hours training • Interviewing substance using individuals • CASI • Data collection routines using ACCESS • Behavioral practice on scheduling calls, mock interviews, follow-up appointment calls • Standard operating procedures • Ethics • Managing difficult persons
Quality Assurance/Supervision • Each interview audiotaped; 15% randomly reviewed by Project Director • Tapes reviewed within 2 weeks and feedback delivered • QA checklist developed for each assessment • Interviewers attend bi-monthly supervision
Assessment Plan • Baseline measures require 1.5 h • Self-report data for drug use and sexual risk behaviors cover a 3-month recall period • Additional resources may provide for re-contact of participants at 3-, 9-months
Demographics/Acculturation • Demographics (Baseline only) • Age, gender, race/ethnicity, education, employment status, income, relationship status, residential stability • Acculturation (Baseline; termination) • Internalized Homonegativity Inventory – personal homonegativity, gay affirmation, morality of homosexuality (Mayfield 2001) • Latino, African Americans use measure to assess language, media and ethnic social relations (Caetano, 1987); parallel measure for Asians (Suinn et al., 1995)
Drug Use MeasuresBaseline, 6-, 12-Months • Addiction Severity Index • Scales tapping 7 areas • 30 day recall for recent drug use • Time Line Follow-Back • Recall of drug use for 3 months prior to assessment point • Periods longer than 3 months unreliable in active drug users
Sexual Behavior MeasuresBaseline, 6-, 12-Months • NIMH Multisite Trial Cooperative Agreement (for heterosexuals), Gorbach’s measures, Behavioral Questionnaire for last 3 months on: • Number and gender of partners • Type of partners (primary, regular, nonexclusive, new) • Knowledge of serostatus of partner • Type and frequency of sexual acts • Frequency and type of condom use in each act • Use of drugs/alcohol during sexual encounters • Risk factors among partners
Sexual Behaviors (cont’d) • Series of questions will investigate role of drug use in exaggerating risk • Facilitate recall of specific, detailed information on type and amount of drug use • Estimate of duration of sexual episode(s) • Abrasions, ulcerations, bleeding • Rougher sex than usual • Whether subject had STD at the time • Partnership calendar will capture specific behaviors in a partnership during the last week
Partnership AssessmentsBaseline, 6-, 12-Months • Partnership Assessment Scale • Concurrency Typology Index • Characteristics of Partnerships • Duration, emotional intensity, resource sharing, cohabitation, sexual frequency, frequency of social interaction, concurrent partnership, level of social integration, place of sexual encounter, source of meeting • Frequency of social interaction (times, modes)
Measuring Partnership Types UNKNOWN PERSON-someone that you had never met before you had sexual contact and never plan to see again ONETIME PARTNER-someone you knew of or had seen before, but you had sexual contact with only one time ACQUAINTANCE- someone you have had sexual contact with more than once, but not on a regular basis, and who you don't socialize with FRIEND- someone you have had sexual contact with more than once, but not on a regular basis, and you normally socialize with
Types of Concurrent Partnerships Primary Partner No Primary Partner “Fuckbuddy” Survival Sex= (Sex for $ & drugs) “1 Night Stands”= “Flings” Co-parent= “Baby’s Mom/Dad” Reciprocal Reactive Separational Transitional Compensatory Experimental Group sex “Bootycall”
Environments • Chart the geographic density of risk establishments within neighborhoods • Types of establishments • Density of MSM and MSM/W at the establishments • Facilitation in providing condoms; prevention • Extent of drug use • Types of sexual risk behaviors • Proportion of risk behaviors under the influence • Frequency of behaviors that resulted in prior HIV/STD infections • Social, sexual, and drug-using contacts that extend from the venue
Mental Health Baseline, 6-, 12-Months • Symptom Check List – 90 – R (Derogatis) • Somatization, OCD, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, psychoticism • Quality and Well-being (RAND Mental Health Inventory) • General positive affect, emotional ties, anxiety, depression, loss of behavioral or emotional control
STD BiomarkersBaseline, 12-Months • HIV testing – rapid test, confirmatory (Elisa) for positives, detuned assay • STD testing – gonorrhea, chlamydia – urine and anal swab using nucleic-acid amplification; syphilis – blood
Ethnography Baseline, 12-Month • 2-hour, semi-structured, in-depth, open-ended interviews with random sample of 40 participants and their sexual partners • Understanding of sexual identity, drug use, HIV risk behaviors, partnerships, social and cultural networks • Probes designed to explore social meanings attached to active drug use and risk behaviors within the relationship, concurrent or monogamous to understand infectious disease status and risk for disease transmission in the context of the participants’ lives
Ethnography Procedure • Pseudonyms used in reporting findings • Interviews analyzed for content; first level coding scheme of re-emerging themes • Themes identified using interview segments that have same labels • Coded by 2 individuals; discrepancies resolved • Text analyzed in Atlas.ti
Data Analysis • Main variables are disease status of HIV, STDs, confirmed at baseline and 12-months • Disease movement slow • Self-report of drug use and psychological status collected at 6-month intervals • Disease status modeled in MSM, MSM/W and their sexual partners at individual level, partnership level, and community/environmental level
Hypothesis 1: Drug Involvement and Infectious Disease • Higher prevalence of HIV/STDs among methamphetamine-using MSM and MSM/W at baseline and 12-months • Methamphetamine users more likely than others to engage in IDU and drug-associated sexual-risk behaviors during the follow-up period • Incidence of HIV infection is higher among methamphetamine users than users of other substances or non-drug using MSM and MSM/W
Hypothesis 2: Sexual Partnerships and Disease Transmission • Methamphetamine users will have more concurrent partnerships than comparison peers • Drug-using MSM, MSM/W will practice high-risk behaviors with non-drug using partners, i.e., a bridge • Partnership dynamics will associate with risky behaviors (no condoms, concurrency) • Pattern and distribution of different types of concurrent partnerships will vary between drug-using MSM and non-drug using MSM/W, with MSM/W at higher concurrency
Hypothesis 3: Modeling the Diffusion of Sexual Risk among Drug Users • Evaluate how the incidence of HIV and STDs reflect the size and connectedness of the sexual networks of each group studied • To determine the impact of sexual network structure in the future transmission of HIV in Los Angeles within and beyond MSM and heterosexual groups
Modeling Approach Schematic of the individual-based modeling software (SimPy) that extends the software to implement the rules by which individuals choose partners, and their behaviors within each partnership
Two Approaches to Modeling • Classical population-level epidemiological models based on differential equations • Pair approximations will model the rate of change of partnerships of different types solved by XPPAUT, which assumes a very large population size • Contrasting approach involves individual-based models of HIV/STD transmission that considers heterogeneity in partnerships
Uses of the Models • Infer the contact network structure from data on partnerships across individuals and the correlation in numbers and types of partnerships and small sub-networks • Implications of the inferred contact network and risk behavior differences between partnership types on disease spread will be simulated • Exploration of the implications of potential biases in our sampling design on our ability to describe the network of contacts, which allows evaluation of the robustness of our solutions
Project Time Line • Months 0-6 • Set-up • Months 6-44 • Recruit cohort; enroll sexual partners; begin ethnography; build databases; ethno papers • Months 18-55 • Conduct follow-up evaluations; data queries and resolutions; Follow-ups end month 55 • Months 48-60 • Data analysis and manuscript publication