Download
1 / 33
340 likes | 528 Views
Psychopathology From Neuropsychology Perspective. Prepared by: Cicilia Evi GradDiplSc ., M. Psi . Psychopathology. Soul ( psycho ) and sickness ( pathos ) = indicating an illness

E N D
PsychopathologyFrom Neuropsychology Perspective Prepared by: CiciliaEviGradDiplSc., M. Psi
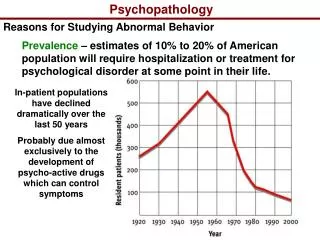
Psychopathology • Soul (psycho) and sickness (pathos) = indicating an illness • Before 19th century people with psychiatric problems were believed to be possessed by evil spirit or bad or morally deficient • 20th century Freud psychopathology as the result of dynamic conflict between conscious and unconscious mental processes
Cont. • Watson behaviorist psychopathology results from prior learning and the treatment must involve the application of learning theory classical and operant conditioning • Kraepelin (1921) discover the neurobiological causes of psychopathology, especially schizophrenia (called as dementia praecox) • Alois Alzheimer found correlation between neuropathological abnormalities and Alzheimer
Cont. • In 1897 Richard von Krafft-Ebbing found that general paresis (now known as syphilis) can cause declining in physical and psychological functioning, culminating in personality changes, disturbed gait, delusions, and then dementia and death. • Syphilis is caused by bacterial infection and has delayed onset of symptoms
Biological Cause • Kraepelin’s team found no reliable biological correlation with psychopathology • Psychological and social factors exist! therefore, we need a balanced approach to the understanding and treatment of psychopathology
The Schizophrenic Disorders • Diagnostic term by EugenBleuler (1911/1950) a debilitating disorder, or, more probably, a group of disorders, that has a lifetime prevalence of 1 – 1,5% (Zigmond et all, 1999) • Major health problems 400,000 people are hospitalized in the US (Black & Andreasen, 1994) • Typically chronic have time when the symptoms were more/less intense, rarely recover permanently
Symptoms • There are 2 types: positive and negative • Positive symptoms and behaviors that are present but should not be delusions, hallucinations, disorganized speech/thoughts • Negative behaviors that are not present but should be taking care of personal hygiene, social interactions • Schizophrenic patients may exhibit one or both types of symptoms
Positive Symptoms • DSM-IV-TR diagnostic criteria • Delusions erroneous beliefs that usually involve a misinterpretation of perceptions or experiences variety of themes: persecutory, referential, somatic, religious, or grandiose • Hard to distinct with a strongly held idea • Bizarre behavior behavior outside the conventional range of behavior for a given context that does not serve any apparent adaptive function
Cont. • Hallucinations perceptual experiences that are not based on sensory stimuli may occur in any sensory modality: auditory, visual, olfactory, gustatory and tactile • Disorganized thoughts (formal thought disorder) disorganization of the form of thinking loose association, unrelated, word salad • Grossly disorganized behavior ranging from childlike silliness to unpredictable agitation
Negative Symptoms • Affective flattening common, characterized by the person’s face appearing immobile and unresponsive, with poor eye contact and reduced body language • Alogia (poverty of speech) manifested in brief, laconic, empty replies have a diminution of thoughts, not unwillingness to speak • Avolition inability to initiate and persist in goal-directed activities sit for a long period of time, show no interest in work or social activities
Multiple Etiologies • Genetic Factors • In twin studies concordance rate is high monozygotic 55% and dizygotic 10% • 15% children who grow up with schizophrenic mothers become schizophrenic • Adoption studies high percentage even the babies are adopted immediately after birth • Not entirely determined by genetic factors!
Cont. • Dopamine Hypothesis • Abnormally increased dopamine activity in the brain is an important factor in schizophrenia • Antipsychotic or neuroleptics block dopamine receptors chlorpromazine (Thorazine) and haloperidol (Haldol) • Different neuroleptic medications block dopamine receptors to different degrees the magnitude of the therapeutic effect of different neuroleptics is proportional with the dopamine blocking effect
Cont. • Problems with the Dopamine hypothesis • (1) the effect is relatively slow, taking weeks this time lag does not fit the hypothesis that dopamine hyperactivity is the cause of schizophrenia; • (2) Diverse response marked reduction to no reduction it is unclear why dopamine hyperactivity should cause such diverse patterns • Only positive symptoms are related to dopamine hyperactivity, while negative symptoms are related to structural abnormalities
Cont. • Refinement of Dopamine hypothesis atypical antipsychotic, block both dopamine and serotonin receptors more effective in treating many schizophrenic patients, esp with negative symptoms • Gross Structural Abnormalities • Microstructural Abnormalities • Abnormalities Revealed by Functional Imaging • Neurological Abnormalities in Schizophrenia
Cont. • Neuropsychological Functioning in Schizophrenia • Symptoms of schizophrenia disrupt attentional processes • Impairments in temporal-lobe (verbal and non-verbal memory) and prefrontal dysfunction (working memory, cognitive flexibility, planning)
Mood Disorders • Formerly termed affective disorders a long-term disturbance of mood as their predominant feature • Major Depressive Disorder • Seasonal Affective Disorder • Bipolar Disorder
Major Depressive Disorder • Characterized by dysphoric (sad, depressed) mood and/or loss of interest and pleasure in nearly all activities associated symptoms include changes in appetite and weight (increase or decrease), sleep disturbance, decreased psychomotor activity, decreased energy, feelings of worthlessness or guilt, difficulty concentrating and making decision, thoughts of death.
MDD cont. • 15% of MDD patients die of suicide • In minority of cases accompanied by delusional thoughts, which congruent with patient’s depressed mood • Vegetative symptoms symptoms that presumed to be more directly related to brain dysfunction incl disturbances in sleep (trouble falling asleep, early awakening, or excessive sleep), loss of appetite, diurnal mood variation and decreased sex drive
Hypothesis of MDD • Monoamine hypothesis of Depression • Abnormally low levels of monoamines play a role in depression • Monoamine neurotransmitters in the brain: catecholamines dopamine, norepinephrine, and indoleamine serotonin • Refinements: catecholamines hypothesis of depression and serotonin hypothesis of depression • Proxac effective in treating the symptoms of MDD (Kramer, 1993)
Hypothesis cont. • Possible endocrine dysfunction in depression • Abnormalities revealed by functional imaging • Genetic Factors • In monozygotic twins the concordance rate is 4 times higher than in dizygotic twins • Genetic cannot entirely account for MDD
Seasonal Affective Disorder • Depressed during winter months, when days are short and nights are long • Possible cause is the disruption of hypothalamus activity involved in the entrainment of normal daily activity rhythm by changes in dark-light onset times • Treatment Light therapy exposing patients to bright light for several hours/day (Rosenthal et al, 1985; Stinson & Thompson, 1990)
Bipolar Disorder • Formerly called as manic-depressive disorder characterized by fluctuation between periods of depression and period of mania, with normal periods interspersed between these episodes • Few hours to several months • In 0.5 – 1% of population (Andreasen & Black, 1996)
Bipolar Disorder cont. • Manic episodes are characterized by a persistently, elevated, expansive or irritable mood, which may include inflated self-esteem, a decreased need for sleep and an increased tendency to talk • Mania may also include flight of ideas, distractibility, increased goal-directed behavior, hypersexuality, and an excessive tendency to engage in pleasurable activities with painful or dangerous sequences (APA, 1994)
Neurochemical Factors • First medication lithium carbonate (Eskalith) dramatically reduces manic symptoms within a matter of days mechanism unknown • Bipolar disorder is more effectively treated by psychoactive medications than any other MDD • Ironically, the therapeutic effectiveness of these medications has yet to reveal very much about the neurochemical basis of the disorder
Genetic Factors • Separate inheritance pathways with MDD • Abnormality in the X chromosome same chromosome for color blindness • No single mechanism of genetic transmission can account for all cases of bipolar disorder
Anxiety Disorders • Characterized by feelings of anxiety and behavioral efforts to cope with these feelings • Four most serious categories of anxiety disorders phobic disorders, GAD, panic disorder and OCD
Simple Phobia • Phobic disorders involve anxiety related to a particular type of object or situation • Phobia may have genetic basis is consistent with the fact that most people with a snake or insect phobia have never been harmed by these animals
Generalized Anxiety Disorder • No particular type of stimulus triggers anxiety a person is plagued by a chronic feeling of anxiety that is not related to anything in particular, a ‘free floating’ anxiety • The most common anxiety disorder 6% in any given population in any given year (Weissman, 1985) neurobiological factors underlying it remain poorly understood
Panic Disorder • Characterized by intermittent but highly intense episodes of anxiety patient describes the anxiety as overwhelming • Misinterpretation of overexcitability of sympathetic NS as an indicator of serious physical condition (e.g., heart attack) makes the person more fearful, further activating sympathetic arousal and so on
OCD • Preoccupying thoughts involuntarily dominate the patient’s thinking • Obsessions often related to a particular theme dirt and contamination, aggression, religion or balance • To deal with this anxiety, patient engages in compulsions behaviors that they cannot keep from performing
Sociopathy • Refer to individuals who behave in a manner that indicates an extreme lack of concern for the immediate or future consequences of their behavior • Callous, selfish, and irresponsible, frequently manipulate and exploit others, exhibit little or no empathy, often engage in illegal behavior, without feeling guilty or remorse, no sense of emotional connection to other people
Sociopathy cont. • Lack of subjective anxiety and fear + absence of autonomic arousal under-arousal of cortex in sociopaths • This could account of why individuals with this disorder often tirelessly seek stimulation
What Can We Do? • Medication can help at first … but patient needs more than that! • Behavioral Therapy • Occupational Therapy • Cognitive – Behavioral Therapy • Family/Support Therapy