Download
1 / 14
140 likes | 232 Views
CONTROLLING COSTS OF HEALTH CARE. Government Policies. The income tax system subsidizes ‘employer-provided’ health insurance The income tax system, until recently, made comprehensive insurance coverage more attractive than ‘catastrophic’ coverage

E N D
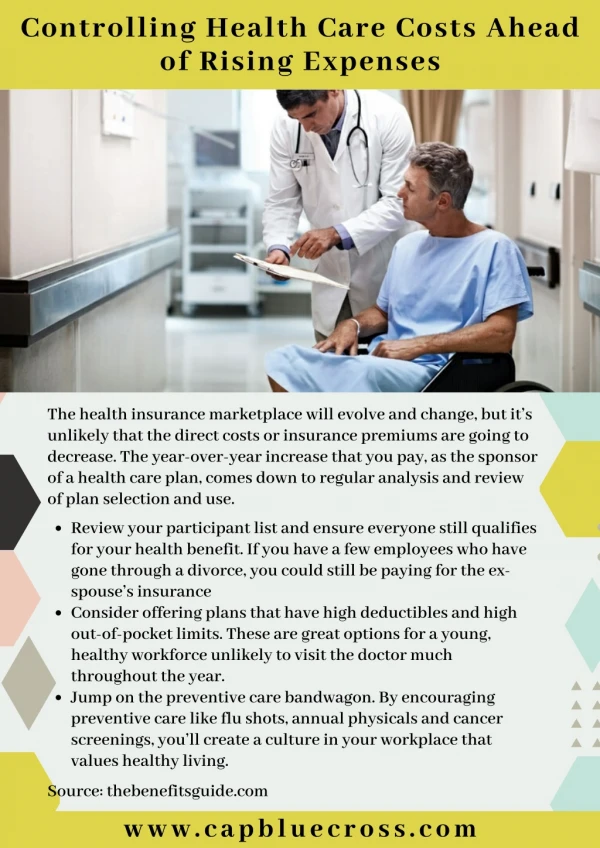
Government Policies • The income tax system subsidizes ‘employer-provided’ health insurance • The income tax system, until recently, made comprehensive insurance coverage more attractive than ‘catastrophic’ coverage • Comprehensive coverage encourages more extensive use of medical services than does catastrophic coverage due to what is known as the effect of ‘moral hazard’.
Medicare • Introduced in 1965 • Created as a ‘third party’ insurer • No restrictions on choice of health care provider • Re-imbursement according to a fee for service schedule • Re-imbursement schedule similar to those of private health insurers (e.g. Blue Cross) • No restrictions of fees set by providers, but re-imbursements limited to the smaller of actual fee charged or the highest fee charged by no more than 75% of providers in market last year • Encouraged provision of all services of benefit to patient without regard to cost
Prospective Payment System • Between 1967 and 1983 Medicare part A annual costs increased from $3 billion to $37 billion • In 1982 Congress authorized a new payment system based on Prospective Payment • In the Prospective Payment system each patient is placed into a Diagnostic Related Group category upon admission. A fixed payment is then made based on this classification without regard to the actual services delivered to this particular patient. • Provides incentives to treat patients a lowest cost consistent with effective treatment • Fundamentally changed the power structure within hospitals
HMOs:Private Market Response to Rising Health Care Costs • Health Maintenance Organizations are first party insurers. • Early HMOs hired their own physicians and operated their own hospitals. Members of HMOs were promised care by these health care providers at no cost beyond their premiums. • HMOs attempt to control costs by structuring incentives for cost control into their contracts with health care providers, coordinating care among health care providers and by controlling access of their policy holders to specialists. • Henry Kaiser operated one of the first large-scale HMOs for his own workers during World War II. • After the war, it was opened to others through the Kaiser-Permanente plan. • For-Profit insurers began to form HMO’s as enrollment in HMOs grew in response to the lower premiums they offered than did third-party insurers. • HMO enrollment grew from 3million in 1970 to more than 80 million by 1999 • The rapid growth of HMO enrollment, together with the introduction of Medicare Prospective Payment is associated with the decline in the rate of growth of health care costs in the late 1980s and early 1990s.
COST DRIVERS Estimated Contributions of Selected Factors to Growth in Real Health Care Spending Per Capita, 1940 to 1990 (percent) Smith, Heffler, and Cutler (1995) Newhouse 1992) Freeland (2000) • Aging of the Population 2 2 2a • Changes in Third-Party Payment 10 13 10b • Personal Income Growth 11–18 5 <23 • Prices in the Health Care Sector 11–22 19 * • Administrative Costs 3–10 13 * • Defensive Medicine and • Supplier-Induced Demand 0 * 0 • Technology-Related Changes • in Medical Practice 38–62 49 >65
COST REDUCTION PROPOSALS • Policy Options and Net Cumulative Impact on National Health Expenditures over One, Five, and 10 Years • billions) • 1 yr 5 yr 10 yr • Producing and Using Better Information • 1. Promoting Health Information Technology $8 $14 –$88 • 2. Center for Medical Effectiveness and • Health Care Decision-Making –$18 –$125 –$368 • 3. Patient Shared Decision-Making –$1 –$4 –$9 • Promoting Health and Disease Prevention • 4. Public Health: Reducing Tobacco Use –$5 –$64 –$191 • 5. Public Health: Reducing Obesity –$3 –$61 –$283 • 6. Positive Incentives for Health $0 –$5 –$19 • Aligning Incentives with Quality and Efficiency • 7. Hospital Pay-for-Performance –$2 –$14 –$34 • 8. Episode-of-Care Payment –$17 –$96 –$229 • 9. Strengthening Primary Care and Care Coordination –$5 –$60 –$194 • 10. Limit Federal Tax Exemptions for • Premium Contributions –$10 –$55 –$131 • Correcting Price Signals in the Health Care Market • 11. Reset Benchmark Rates for • Medicare Advantage Plans –$3 –$20 –$50 • 12. Competitive Bidding –$7 –$42 –$104 • 13. Negotiated Prescription Drug Prices –$3 –$16 –$43 • 14. All-Payer Provider Payment Methods and Rates $2 –$23 –$122 • 15. Limit Payment Updates in High-Cost Areas –$4 –$43 –$158
Senate Bill • Re: Center for Medical Effectiveness: Create working group to identify best practices and disseminate information—no authority to implement incentives • Re: Public health: Authorizes public health investment fund…no incentives to reduce use of tobacco and of soft drinks • Re:Better alignment of incentives for quality and efficiency..funds for consumer operated non-profit HMOs; tax on ‘Cadillac’ plans • Re: Correcting Price Signals—reduce payments for Medicare Advantage Plans; no authority to limit payments to high cost areas; no authority to negotiate drug prices
Cost Savings of a Single Payer System • Insurance Overhead was 1.3% in Canada • Insurance Overhead was 11.7% among U.S. Private Insurers • Estimated fraction of total medical expenditures devoted to administration: U.S.---31% Canada-16.7% Cutting administrative costs of provision of medical care by ½ would save more than all of the potential cost savings identified and evaluated by the Commonwealth Fund
Incentives for Consumers • Comprehensive Insurance coverage (low deductibles and low co-payments) discourages price shopping and encourages use of health care provider services • Evidence from Rand Medical Insurance Experiment: People with 0 deductibles spent 30% more on medical services than did people with $1,000 deductibles • Republican Proposal: make medical savings accounts exempt from taxation for people who select Catastrophic Insurance ( high deductible policies). • Democratic Party Objection: Only people of above average health will choose catastrophic insurance when both catastrophic and comprehensive policies are available with the same tax advantages. This will raise the cost of comprehensive policies. • Is health care like merchandise sold in supermarkets? Will people price shop in order to save money? • According to the Rand Study, the answer is, “No”. • Furthermore, for high ticket items—i.e., hospital stays, people with catastrophic insurance went to the hospital as frequently as did people with comprehensive coverage.
“Bending the Curve” • Policies recommended by the Commonwealth Fund and considered in the recent health reform legislation might lower the cost of health care, but • They won’t reduce the rate of growth of health care expenditures • With a rate of growth in expenditures of 5%/year a 10% reduction in costs this year would be wiped out in 2 years. • To reduce the rate of growth of health care expenditures we will need to adopt policies that reduce the pace of development of new treatment modalities and reduce the rate at which those new modalities that become available are utilized. • Is anyone willing to forego the benefits of future medical advances in order to save money now?