Download
1 / 1
10 likes | 103 Views
KEY PAPERS/ ACKNOWLEDGEMENTS. 1 - BACKGROUND. Judd A et al. Morbidity, mortality, and response to treatment by children in the United Kingdom and Ireland with perinatally acquired HIV infection during 1996-2006: planning for teenage and adult care . Clin Infect Dis 2007,45:918-924.

E N D
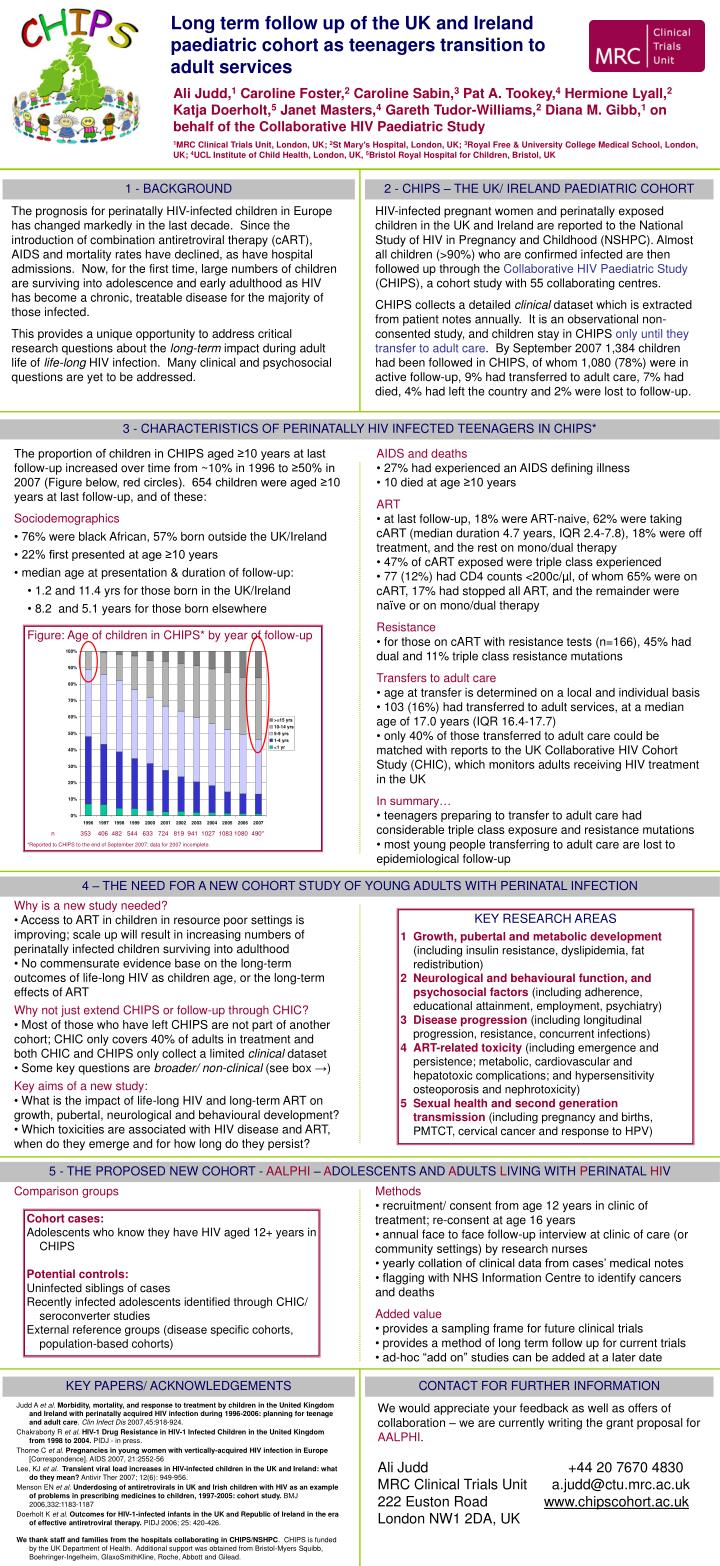
KEY PAPERS/ ACKNOWLEDGEMENTS 1 - BACKGROUND Judd A et al.Morbidity, mortality, and response to treatment by children in the United Kingdom and Ireland with perinatally acquired HIV infection during 1996-2006: planning for teenage and adult care. Clin Infect Dis 2007,45:918-924. Chakraborty R et al. HIV-1 Drug Resistance in HIV-1 Infected Children in the United Kingdom from 1998 to 2004. PIDJ - in press. Thorne C et al. Pregnancies in young women with vertically-acquired HIV infection in Europe [Correspondence]. AIDS 2007, 21:2552-56 Lee, KJ et al. Transient viral load increases in HIV-infected children in the UK and Ireland: what do they mean? Antivir Ther 2007; 12(6): 949-956. Menson EN et al. Underdosing of antiretrovirals in UK and Irish children with HIV as an example of problems in prescribing medicines to children, 1997-2005: cohort study. BMJ 2006,332:1183-1187 Doerholt K et al. Outcomes for HIV-1-infected infants in the UK and Republic of Ireland in the era of effective antiretroviral therapy. PIDJ 2006; 25: 420-426. We thank staff and families from the hospitals collaborating in CHIPS/NSHPC. CHIPS is funded by the UK Department of Health. Additional support was obtained from Bristol-Myers Squibb, Boehringer-Ingelheim, GlaxoSmithKline, Roche, Abbott and Gilead. The prognosis for perinatally HIV-infected children in Europe has changed markedly in the last decade. Since the introduction of combination antiretroviral therapy (cART), AIDS and mortality rates have declined, as have hospital admissions. Now, for the first time, large numbers of children are surviving into adolescence and early adulthood as HIV has become a chronic, treatable disease for the majority of those infected. This provides a unique opportunity to address critical research questions about the long-term impact during adult life of life-long HIV infection. Many clinical and psychosocial questions are yet to be addressed. Comparison groups • The proportion of children in CHIPS aged ≥10 years at last follow-up increased over time from ~10% in 1996 to ≥50% in 2007 (Figure below, red circles). 654 children were aged ≥10 years at last follow-up, and of these: • Sociodemographics • 76% were black African, 57% born outside the UK/Ireland • 22% first presented at age ≥10 years • median age at presentation & duration of follow-up: • 1.2 and 11.4 yrs for those born in the UK/Ireland • 8.2 and 5.1 years for those born elsewhere CONTACT FOR FURTHER INFORMATION 2 - CHIPS – THE UK/ IRELAND PAEDIATRIC COHORT We would appreciate your feedback as well as offers of collaboration – we are currently writing the grant proposal for AALPHI. Ali Judd +44 20 7670 4830 MRC Clinical Trials Unit a.judd@ctu.mrc.ac.uk 222 Euston Road www.chipscohort.ac.uk London NW1 2DA, UK • Methods • recruitment/ consent from age 12 years in clinic of treatment; re-consent at age 16 years • annual face to face follow-up interview at clinic of care (or community settings) by research nurses • yearly collation of clinical data from cases’ medical notes • flagging with NHS Information Centre to identify cancers and deaths • Added value • provides a sampling frame for future clinical trials • provides a method of long term follow up for current trials • ad-hoc “add on” studies can be added at a later date • AIDS and deaths • 27% had experienced an AIDS defining illness • 10 died at age ≥10 years • ART • at last follow-up, 18% were ART-naive, 62% were taking cART (median duration 4.7 years, IQR 2.4-7.8), 18% were off treatment, and the rest on mono/dual therapy • 47% of cART exposed were triple class experienced • 77 (12%) had CD4 counts <200c/µl, of whom 65% were on cART, 17% had stopped all ART, and the remainder were naïve or on mono/dual therapy • Resistance • for those on cART with resistance tests (n=166), 45% had dual and 11% triple class resistance mutations • Transfers to adult care • age at transfer is determined on a local and individual basis • 103 (16%) had transferred to adult services, at a median age of 17.0 years (IQR 16.4-17.7) • only 40% of those transferred to adult care could be matched with reports to the UK Collaborative HIV Cohort Study (CHIC), which monitors adults receiving HIV treatment in the UK • In summary… • teenagers preparing to transfer to adult care had considerable triple class exposure and resistance mutations • most young people transferring to adult care are lost to epidemiological follow-up HIV-infected pregnant women and perinatally exposed children in the UK and Ireland are reported to the National Study of HIV in Pregnancy and Childhood (NSHPC). Almost all children (>90%) who are confirmed infected are then followed up through the Collaborative HIV Paediatric Study (CHIPS), a cohort study with 55 collaborating centres. CHIPS collects a detailed clinical dataset which is extracted from patient notes annually. It is an observational non-consented study, and children stay in CHIPS only until they transfer to adult care. By September 2007 1,384 children had been followed in CHIPS, of whom 1,080 (78%) were in active follow-up, 9% had transferred to adult care, 7% had died, 4% had left the country and 2% were lost to follow-up. Long term follow up of the UK and Ireland paediatric cohort as teenagers transition to adult services Ali Judd,1 Caroline Foster,2 Caroline Sabin,3 Pat A. Tookey,4 Hermione Lyall,2 Katja Doerholt,5 Janet Masters,4 Gareth Tudor-Williams,2 Diana M. Gibb,1 on behalf of the Collaborative HIV Paediatric Study 1MRC Clinical Trials Unit, London, UK; 2St Mary’s Hospital, London, UK; 3Royal Free & University College Medical School, London, UK; 4UCL Institute of Child Health, London, UK, 5Bristol Royal Hospital for Children, Bristol, UK 3 - CHARACTERISTICS OF PERINATALLY HIV INFECTED TEENAGERS IN CHIPS* Figure: Age of children in CHIPS* by year of follow-up n 353 406 482 544 633 724 819 941 1027 1083 1080 490* *Reported to CHIPS to the end of September 2007; data for 2007 incomplete. 4 – THE NEED FOR A NEW COHORT STUDY OF YOUNG ADULTS WITH PERINATAL INFECTION • Why is a new study needed? • Access to ART in children in resource poor settings is improving; scale up will result in increasing numbers of perinatally infected children surviving into adulthood • No commensurate evidence base on the long-term outcomes of life-long HIV as children age, or the long-term effects of ART • Why not just extend CHIPS or follow-up through CHIC? • Most of those who have left CHIPS are not part of another cohort; CHIC only covers 40% of adults in treatment and both CHIC and CHIPS only collect a limited clinical dataset • Some key questions are broader/ non-clinical (see box →) • Key aims of a new study: • What is the impact of life-long HIV and long-term ART on growth, pubertal, neurological and behavioural development? • Which toxicities are associated with HIV disease and ART, when do they emerge and for how long do they persist? KEY RESEARCH AREAS 1 Growth, pubertal and metabolic development (including insulin resistance, dyslipidemia, fat redistribution) 2 Neurological and behavioural function, and psychosocial factors (including adherence, educational attainment, employment, psychiatry) 3 Disease progression (including longitudinal progression, resistance, concurrent infections) 4 ART-related toxicity (including emergence and persistence; metabolic, cardiovascular and hepatotoxic complications; and hypersensitivity osteoporosis and nephrotoxicity) 5 Sexual health and second generation transmission (including pregnancy and births, PMTCT, cervical cancer and response to HPV) 5 - THE PROPOSED NEW COHORT - AALPHI – ADOLESCENTS AND ADULTS LIVING WITH PERINATAL HIV Cohort cases: Adolescents who know they have HIV aged 12+ years in CHIPS Potential controls: Uninfected siblings of cases Recently infected adolescents identified through CHIC/ seroconverter studies External reference groups (disease specific cohorts, population-based cohorts)