Download
1 / 17
180 likes | 737 Views
Systems of Classification. Year 12 Psychology Unit 4 Area of Study 2 (chapter 11 , page 558 ). Systems of Classification of Mental Conditions & Disorders. Classification: organising items into groups based on their shared characteristics. Two main classifications of mental illness:

E N D
Systems of Classification Year 12 Psychology Unit 4 Area of Study 2(chapter11, page 558)
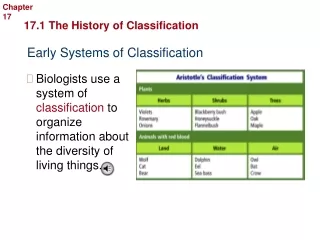
Systems of Classification of Mental Conditions & Disorders • Classification: organising items into groups based on their shared characteristics. • Two main classifications of mental illness: • Categorical approaches: organises mental disorders into categories, each with specific symptoms and characteristics. • Dimensional approaches:classifies symptoms quantitatively in terms of their severity, or ‘how much’ (i.e. ranking). • Often both are used to provide an overall assessment.
Categorical Approach • Diagnosis involves a comparison of patients symptoms to the listed symptoms within each category: • Check your patient’s list against the lists in the DSM-IV to find a fit – then make diagnosis. • Assumes that mental disorders can be diagnosed from specific symptoms reported by the patient or observed by the professional. • Thoughts feelings and behaviours can be categorised – certain categorisation relates to specific disorders. • There are distinct sub categories within each disorder. • All or nothing – they either have it or they don’t. You can’t ‘kind of’ have schizophrenia. • The system must be valid and reliable.
Diagnostic & Statistical manual of Mental Disorders • The system most widely used by mental health professionals throughout the world to identify and classify mental illnesses for the purposes of diagnosis. • More commonly called the DSM. • An important feature of the DSM-5 is that it does not suggest causes of specific disorders unless a cause can be definitely established: • It simply names the disorders anddescribes them in specific terms.
DSM-5 • 365 disorders comprehensively described (one for every day of the year!). • Grouped into 17 categories. • Diagnosis matches patient symptoms to the disorder symptoms. • Symptoms are considered characteristics of disorders so looking at these enables diagnosis: • Inclusion criteria: symptoms that must be present for diagnosis; • Exclusion criteria: symptoms that must not be present; • Polythetic criteria: only some symptoms need to be present for diagnosis – e.g. “3 of the following 8.” • Provides info on the typical course of the disorder. • http://www.dsm5.org/about/Pages/faq.aspx
DSM-5 (axes) • Axis I: clinical disorders. Symptoms that cause distress or significantly impair social or occupational functioning (such as anxiety disorders, depression). SEE BOX 11.5 ON PAGE 562. • Axis II: personality disordersandmental retardation. Chronic and enduring problems that generally persist throughout life and impair interpersonal or occupational functioning (such as multiple personality disorder). • Axis III: general medical condition. Physical disorders that may be relevant to understanding or treating a psychological disorder. • Axis IV: psychosocial and environmental problems (such as interpersonal stressors and negative life events). Factors that may affect the diagnosis, treatment and prognosis (prediction of the course of a disease) of psychological disorders. • Axis V: global assessment of functioning. The individual's overall level of functioning in social, occupational and leisure.
International Classification of Diseases & Related Health Problems • Commonly known as ICD-10. • Diagnosis and classification of mental disorders based on recognised symptoms. • Includes detailed description of each disorder listed. • Identifies symptoms that indicate the presence of a disorder. • Original text covered all medical practice with mental disorders covered in Chapter V: • Chapter V now printed as a separate book. • Less detailed than the DSM –IV.
Strengths of Categorical Approaches Activity: 11.14 • Allows clear-cut diagnosis of mental disorders(this is the main purpose of the categorical approach). • Enhances communication between professionals by providing a common language: • Diagnostic labels can convey a large amount of information quickly and conveniently. • Very comprehensive list of disorders, symptoms and additional disorder information. • User-friendly system: • This fits with the ‘yes/no’ approach used by most healthcare professionals.
Limitations of Categorical Approaches • Historically low inter-rater reliability (different conclusions reached by different professionals): • Much better now with DSM-IV-TR and ICD-10: up to 70% agreement between mental health professionals • BUT still as much as 30% disagreement in classification of people with mental disorders and much lower inter-rater reliability for personality disorders. • Lots of overlap between symptoms can make diagnosis difficult. • Substantial loss of valuable clinical information: individuality of the patient becomes overlooked when they are simply categorised. • Categorisation and ‘labels’ can result in stigma.
Dimensional Approach • Determines how much of a characteristic is normal; numerical values are assigned to each characteristic score: • Measure all characteristics and the combination of scales that are statistically extreme might point to the type of illness being suffered. • Dimension: cluster of related psychological/behavioural characteristics that occur together. • Quantifies symptoms and other characteristics with numerical values: • These values are compared with the statistically ‘normal’ expected values for each characteristic;
Scales on the MMPI • Hs Hypochondriasis Concern with bodily symptoms • D Depression Depressive Symptoms • HyHysteria Awareness of problems and vulnerabilities • Pd Psychopathic Deviate Conflict, struggle, anger, respect for society's rules • MF Masculinity/Femininity Stereotypical masculine or feminine interests/behaviors • Pa Paranoia Level of trust, suspiciousness, sensitivity • Pt Psychasthenia Worry, Anxiety, tension, doubts, obsessiveness • Sc Schizophrenia Odd thinking and social alienation • Ma Hypomania Level of excitability • Si Social Introversion People orientation
MMPI – the t scores • The t-score represents how statistically different each scale result is from the mean/average t-score (50): • Is the difference big enough to be significant? • Statistical normality is the key here! • Lower scores equate to lower impairment; • Higher scores equate to higher impairment. • SEE FIGURES ON PAGES 574 & 575
Strengths of Dimensional Approaches • Take into account a wider range of factors than categorical approaches. • More detailed information on each symptom (quantifying): • Not just a label, an assessment of the degree or extent of the illness. • Reduced stigma as labelling not used: • Instead a profile is created; • Patients are viewed as having extreme variants of common traits, rather than being labelled as completely ‘different’.
Limitations of Dimensional Approaches Activity: 11.16 & 11.17 • There is no standardised inventory to compare individual scores to, thus diagnosis is difficult. • Mental health professionals need to create the questions and scales themselves (may have to rate a client on up to different 40 dimensions). • This makes using dimensional approaches a very time-consuming and difficult process. • Disagreement among professions and researchers on the number of dimensions that suitably represent the wide range of mental disorder symptoms people can experience: • If there are too many dimensions, assessment could become overcomplicated.