Download
1 / 47
480 likes | 829 Views
Acute unilateral red eye. Dr. Anthony Hall MD, FRA NZ CO. differential diagnosis of the unilateral red eye. Eyelid Conjunctiva Conjunctivitis Cornea Corneal foreign body/ulcer Infectious keratitis Sclera Anterior chamber Iritis Angle closure glaucoma Orbit. Eyelid.

E N D
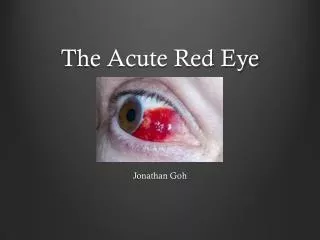
Acute unilateral red eye Dr. Anthony Hall MD, FRANZCO
differential diagnosis of the unilateral red eye • Eyelid • Conjunctiva • Conjunctivitis • Cornea • Corneal foreign body/ulcer • Infectious keratitis • Sclera • Anterior chamber • Iritis • Angle closure glaucoma • Orbit
Acute lid problems Chalazion Preseptal cellulitis
Chalazion • Obstructed and infected and inflamed meibomian gland • Unilateral, unifocal lid swelling
Chalazion – initial treatment • Topical antibiotics • + oral if associated cellulitis • Hot compresses • If fails then surgery
Chalazion – surgical treatment • LA • Lid everted • Chalazion incised form tarsal surface
Preseptal cellulitis • Acutely unwell • Swollen, tender red eyelid • No orbital signs • No proptosis, visual loss, movement problems
The orbital septum divides the eyelid from the orbit Orbital vs preseptal cellulitis
Conjunctivitis • Viral • Watery discharge • URTI • Allergic • Itch • Stringy discharge • Atopic patient • Usually bilateral!!
Viral conjunctivitis • URTI • Acute pain, redness, and watery discharge • Normal pupil • Normal VA • Normal cornea • Management
Allergic conjunctivitis • Atopy • Sub-acute irritation, itch, redness, and stringy discharge • Normal pupil • Normal VA • Normal cornea
Keratitis • Suspect if • Corneal fluorescein stain (dendritic) • Focal corneal swelling • Past history HSV/VZV • Contact lens wear • Post trauma
Keratitis management • HSV • Topical aciclovir till epithelium healed
Keratitis management • Bacterial • Intensive topical antibiotics
Corneal foreign body/ulcer • Suspect if • History of grinding etc • Fluorescein staining • Corneal/subtarsal foreign body • Always evert eyelid
Management of corneal FB • Topical LA • Remove fb with 23 G needle • Oc Chloro and pad 24 hrs
Corneal ulcer • Without Fluorescein: • Underlying cornea is clear - iris details are seen
Trauma • Hyphaema or corneal abrasion may follow trauma • In this setting beware of • Keratitis • Perforation
Iritis(acute anterior uveitis) • Inflammation confined primarily to the iris and anterior chamber • Resolving totally within three months • (not associated with other significant anterior or posterior segment pathology)
pain redness photophobia epiphora Iritis - symptoms
Iritis - signs • ciliary flush • small irregular pupil • AC cells and flare • keratic precipitates • hypopyon • iris nodules • spill over vitritis
B 27 related diseases • Ankylosing spondylitis • Psoriatic arthritis • Reiters syndrome (reactive arthritis) • Inflammatory bowel disease associated arthropathy
Sarcoidosis • Multisystem granulomatous disease • 90% lung • 90% lymph node • 25-50% joint involvement • 25% skin • 25% eye
Syphilis • Primary • 4-6 weeks of ulcer • Secondary • 2-4 months • Skin rash and lymphadenopathy • Eye and CNS involvement • Latent/tertiary • CVS and CNS
Viral • Suspect if • History of simplex or zoster • Chronic course • Iris changes • High pressure • Keratitis (old or new)
Most important Clinical History Family history Examination Less important HLA B 27 Sarcoidosis CXR ACE Syphilis serology Investigation of AAU
Principles of management of Iritis • Determine the underlying cause • Control the inflammation • Detect and control ocular complications of • the inflammation • the treatment
How to control the inflammation • Adequate high potency topical steroids • Sub conjunctival steroids • Oral steroids • Aggressive dilation • Regular and close review
Acute angle closure glaucoma • Unusual • Severe pain • Profound visual loss • Cloudy cornea • Fixed mid position pupil • Treatment • iridotomy
Orbital cellulitis • Pre septal • Acute lid swelling • No chemosis, visual loss or eye movement disorder • Secondary to trauma, chalazia, lacrimal sac disease • Orbital • Lid swelling • Chemosis, visual loss, eye movement abnormalities • Secondary to sinus disease
Pre septal Orbital
Treatment Pre septal Orbital Image Drain sinus disease Antibiotics Drain orbital disease • Antibiotics
History Ocular Previous episodes CL wear Trauma Systemic Auto-immune disease Recent URTI Examination VA Cornea Pupil Conjunctiva Key steps in the diagnosis of the unilateral red eye