Download
1 / 16
160 likes | 315 Views
Case report no. 9. Recurrence of amyloid in a kidney allograft. Eva Honsová Institute for Clinical and Experimental Medicine Prague, Czech Republic. Clinical history. A 55-year-old man was admitted to the hospital for severe hypertension in 1989.

E N D
Case report no. 9.Recurrence of amyloid in a kidney allograft Eva Honsová Institute for Clinical and Experimental Medicine Prague, Czech Republic
Clinical history • A 55-year-old man was admitted to the hospital for severe hypertension in 1989. • He was well until half a year before when slowly progressing peripheral edema appeared. • He didn’t consult his practitioner until he began to suffer from severe headaches with nausea, and blurred vision. • 210/130mmHg • proteinuria 6g/day, S-Cr level was 296umol/l(3,3mg/dl) • there was a 10 times higher level of antibodies against streptolysin O (ASLO). • A renal biopsy was performed with clinical diagnosis of postinfectious glomerulonephritis.
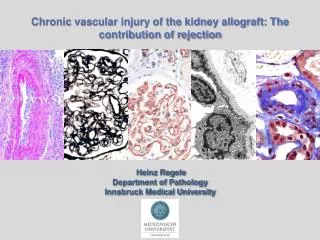
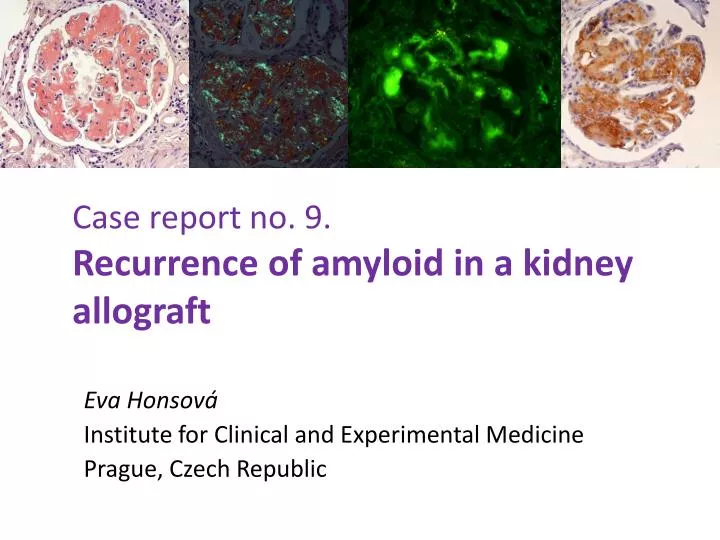
Native kidney biopsy sample (from 1989)IF: Igs negative, C3 negat., kappa, lambda: negat. PAS staining Congo red
Dg: Amyloidosis of an uncertain type. • Extensive searching for some disease associated with amyloidosis • 2 nodules in the liver; biopsy unsuccessful • No evidence of inflammatory disease • No evidence of plasma cell dyscrasia • No other disease in addition to DM type II • Half a year later: viral respiratory illness; kidney function rapidly declined and hemodialysis was begun.
Family medical history Both parents dead (mother: 40, abdominal tumor; father: 77, DM, IHD; sister: 7, car accident) 2 children, a son and a daughter: healthy No evidence of kidney disease • Because of uncertain biological potential of liver lesions, he was not included in the waiting list. • Liver masses were stable for 3 years. • Patient´s data were reevaluated, 6 years after kidney failure he underwent kidney transplantation.
Kidney graft had excellent function for the following 15 years. • No kidney graft biopsy was performed. • Recently, proteinuria was revealed and a kidney graft biopsy was performed with clinical suspicion of diabetic nephropathy and chronic rejection.
Graft biopsy sampleIF: C4d negative; Igs negative; C3,C1q: negative; kappa:negative; lambda: weakly positive, AA:neg.
GGraft biopsy sample, IF & IH detection fibrinogen A r Genetic studies were performed and mutation in the fibrinogen gene was confirmed (Glu526Val)
Follow-up • No change in immunosuppressive treatment • S-Cr 178μmol/l (2.01mg/dl) • PU 3.6g/day • DM under control • Recently, genetic analysis for his 2 children was offered
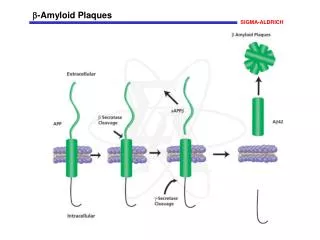
Diagnosis of the type of amyloidosis The most common types: AA+AL AA (commercial antibodies) AL(low reactivityof commercial Abs in paraffinsections) Hereditary amyloidoses: more frequently recognized, are gaining in clinical importance. Autosomal dominant, variable penetrance, family history is lacking, clinical manifestation at older ages, therefore the correct diagnosis is challenging Each type requires different therapy, dg must be based on identification of the protein
Hereditary fibrinogen A amyloidosis • Mutation in Fibrinogen Aα-chain gene was first described by Benson et al. in 1993 • most frequent hereditary amyloidosis in the UK and also in Europe • All cases: renal biopsy samples with massive and exclusively glomerular amyloid deposits • Median age of presentation: 55years • Fibrinogen: produced exclusively by the liver • Kidney transplantation alone associated with rapid recurrence of amyloid • Liver or combined liver and kidney transplantation
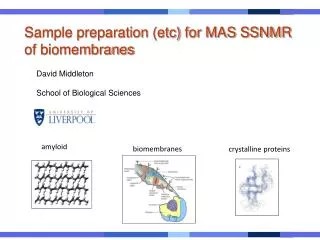
Fascinating story of amyloidosis • Not all of patients with „preconditions“ suffer from amyloidosis • Genetic factors, different types of degradation • Per Westermark: different point of view • Comparison with prion diseases: change in the protein structure • In experiments, amyloid enhancing factor • Amyloid fibrils were identified as the basis of AEF • Prion diseases are transmissible by food
Is amyloidosis transmissible? • Yes, very probably • Westermark GT, Westermark P. Serum amyloid A and protein AA: molecular mechanisms of a transmissible amyloidosis. FEBS Lett. 2009;583:2685-2690. • AA amyloidosis is transmissible in several animal experimental models • AA amyloid can occur in human food (ducks, geese: pate de foie gras) • AA amyloidosis is transmissible by blood monocytes • Will we change the management of patients at risk of amyloidosis?