Download
1 / 11
120 likes | 253 Views
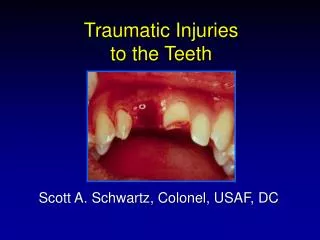
Congenital & Traumatic conditions أد مسعد السيسي. Congenital. Aplasia : Complete absence of the middle ear CD Hearing Aid Ossicular : Absence Deformity Fixation CD Ossiculoplasty i.e surgical reconstruction of the ossicular chain Wall deheiscence :

E N D
Congenital & Traumatic conditions أد مسعد السيسي
Congenital Aplasia: Complete absence of the middle earCD Hearing Aid Ossicular: • Absence • Deformity • Fixation CD Ossiculoplastyi.e surgical reconstruction of the ossicular chain Wall deheiscence : Floor : exposure of the jagular bulb injuru of the jagularbilb during ear operations Facial canal: injury of the facial Nerve during ear operations
0 0 Definition: Trauma due to rapid increase of atmospheric pressure Non infective inflammation due to relatively negative Intratympanic pressure Physiology: At rest : the middle ear pressure is equal to the atmospheric pressure Why? Because the ET is opening during swallowing and yawning During airplane ascent: The atmospheric pressure is decreased middle ear pressure becomes relatively higher than the atmospheric pressure Air outflow from the middle ear through the ET the pressure in the ME becomes equal to the atmospheric pressure During Air plane descent( And diving) The atmospheric pressure increases pressure in the middle ear becomes relatively lower than the atmospheric pressure Air inflow to the middle ear ( during swallowing) pressure in the middle ear becomes relatively lower than the atmospheric pressure Negative positive Negative positive Negtive positive
Otiticbarotraumaoccurs when the ET fails to open during descent in a non pressurized plane or during diving ET obstruction may be due to: Sleep during descent ET obstruction In mild cases : retracted Drum In moderate cases: effusion ( or hemotympanum) In severe cases: drum rupture +VE -VE
واحد نازل من الطيارة عنده الم بالاذن وتقل في السمع Symptoms: • History of flying or diving • Earache • Hearing loss Signs: • Otoscopic: -Retracted drum -Sgns of middle ear effusion - Reupture drum • Tunning fork: conductive deafness Investigations: PTA: Conducive deafness ( Air Bone gap) Tympanometry: Type C : in retracted drum Type B: in middle ear effusion Air Bone Gap Type C Type B
Prophylaxis: • Avoid flying or diving with nasal obstruction • Avoid sleep during descent • Try to open the ET by: Frequent swallowing & chewing gum Valsalvamanoeuvre Vasoconstrictor nasal drops TTT • Retracted Drum Vasoconstrictor nasal drops Valsalvamanoeuvre - ME Effusion Myringotomy • Rupture Drum conservative treatment for 3 months ( see truamatic drum perforation) • Myringoplasty if healing fails after 3 months
Ossicular disruption Etiology: • Head trauma : with or without temporal bone fracture • Ear operations; e.gmyringoplasty, stapedectomy Symptoms: - History of trauma -Hearing loss, tinnitus Signs • Drum is intact or ruptured • Tunnng fork test: conductive deafness Investigations: • PTACD • Tympanometry( if the drum is intact) Type Ad • TTT: osiculoplasty
Longitudinal temporal bone fracture Etiology: - Severe trauma to the head e.g fall from a height or motor car accident Incidence: -more common than transvrse temporal bone fracture 4:1 Pathology • The fracture line is parrallel to he longtudinal axis of temporal bone it passes in the roof of external canal and middle ear and then passes anterior to the VII nerve canal
CP: History of trauma Otoscopic: • Laceration of the skin of the external canal • Rupture drum • Bloody otorrhea • CSF otorrhea Tuning fork tests: CD Facial nerve Paralysis is not common with this type of fracture but with transverse type • Investigations: -CT scan -PTA
Antibiotics Avoid ear wash Avoid entry of water into the ear Avoid ear drops Avoid forcible nose blowing Treatment: Conservative: Similar to rupture drum CSF otorrhea • Prophylactic antibiotics • Bed rest with head elevated • Avoid straining • Cover the ear with sterile dressing Surgical: If conservative measures fail - Myringoplasty • Ossiculoplasty • Repair of CSF leak • Facial nerve paralysis Reconstruction of the ossicles After 3 month Repair of tympanic membrane perforation by a graft
Transverse fractures differs from longitudinal fracture How?