Download
1 / 31
310 likes | 380 Views
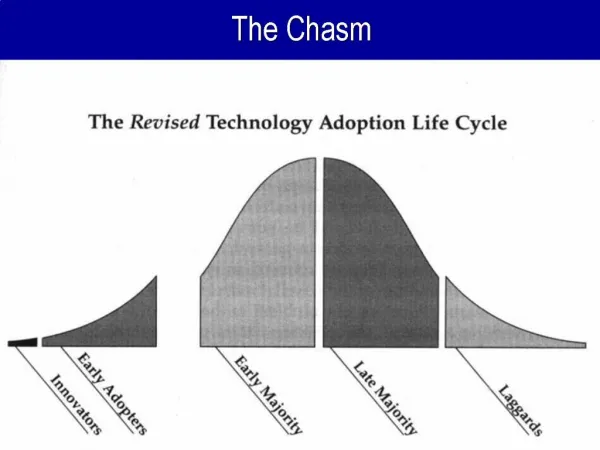
The Quality Chasm in the Behavioral Health Treatment For America's Youth. Michael L. Dennis, Ph.D. Chestnut Health Systems Normal, IL

E N D
The Quality Chasm in the Behavioral Health Treatment For America's Youth Michael L. Dennis, Ph.D. Chestnut Health Systems Normal, IL Presentation for the 26th Annual Children’s Mental Health Research & Policy Conference, Tampa, FL, Mark 3-6, 2013. Hosted by the University of South Florida’s The Department of Child & Family Studies and The Institute for Translational Research in Adolescent Behavioral Health (National Institute of Drug Abuse Grant no. R25DA031103). This presentation uses data from NIDA grants no. R01 DA15523, R37-DA11323, R01 DA021174,, CSAT contract no. 270-12-0397, Library of Congress contract no. LCFRD11C0007 and several public data sets. The author would like to thank Christy Scott, Barb Estrada, Rodney Funk, Lilia Hristova, , Brook Hunter, Rachel Kohlbecker, Lisa Nicholson, and Belinda Willis for their assistance in preparing this presentation. The opinions expressed are those of the author and do not reflect positions of the government. The presentation is available electronically at www.chestnut.org/li/posters . Please address comments or questions to the author at mdennis@chestnut.org or 309-451-7801. .p
The Goals of this Presentation are to Examine: • The quality chasm in behavioral health care, including the low rates of treatment access and engagement, including evidence of health disparities by gender, race, age and involvement in the juvenile justice system. • The prevalence and co-morbidity of internalizing and externalizing mental health disorders, substance use disorders, and crime/violence including how they vary with age • The general factors associated with better outcomes in terms of reduced mental health, substance use and illegal activities
Size & Overlaps of Mental Health and Substance Use Disorder Populations (in millions) Very Low Rates of Treatment Participation • More MH than SUD Comorbidity 15% of those with MH but 71% of those with SUD Source: Institute of Medicine (2005) Improving the quality of health care for mental health and substance-use conditions. Crossing the Quality Chasm Series. Washington, DC: Author
Quality Chasm in Treatment (in millions) Low rates of Identifying Comorbidity Low rates of Cont. Care Low rates of Treatment Compliance Source: Institute of Medicine (2005) Improving the quality of health care for mental health and substance-use conditions. Crossing the Quality Chasm Series. Washington, DC: Author
Problems and Treatment Participation Rates Vary by Age Few Get Treatment: 1 in 20 adolescents, 1 in 18 young adults, 1 in 11 adults Over 88% of adolescent and young adult treatment and over 50% of adult treatment is publicly funded Source: SAMHSA 2010. National Survey On Drug Use And Health, 2010 [Computer file]
Potential to Improve Identification by Screening for SUD in more sites ACA’s expansion of School Based Health Centers present a major opportunity to close the gap Rise of Workplace Wellness programs with health risk assessments Source: SAMHSA 2010. National Survey On Drug Use And Health, 2010 [Computer file]
Less than 80% of the Clients Engage in Treatment for 45 days or more (ONC measure of quality) Source: Office of Applied Studies 2009 Discharge – Treatment Episode Data Set (TEDS)
Less than Half of the Clients Stay in Treatment the 90 days Recommended by Research Source: Office of Applied Studies 2009 Discharge – Treatment Episode Data Set (TEDS)
Data on 29,782 clients from 230 local evaluations in2011 SAMHSA/CSAT GAIN Data Set (89% with 1+ follow-up) NH WA ME MT VT ND MN OR MA NY ID WI SD WY MI RI PA IA NE CT OH NJ IN NV DC UT IL CA CO WV VA DE KS MO KY MD NC TN AR OK AZ NM SC GA GU AL MS TX LA FL AK VI HI PR AAFT ART ATDC ATM BIRT CYT DC EAT FDC JTDC OJJDP ORP RF-JDC SCY TCE YORP
Primary Substance by Age SAMHSA 2011 GAIN Summary Analytic Data Set (n=27,716)
Past Year Substance Severity by Age SAMHSA 2011 GAIN Summary Analytic Data Set (n=29,358)
Tobacco Diagnosis by Age SAMHSA 2011 GAIN Summary Analytic Data Set (n=27,384)
Mental Health Disorders by Age SAMHSA 2011 GAIN Summary Analytic Data Set (n=29,684)
Type of Crime by Age * Violent crime includes assault, rape, murder, and arson. ** Other crime includes vandalism, possession of stolen goods, forgery, and theft. SAMHSA 2011 GAIN Summary Analytic Data Set (n=29,377)
Severity of Victimization by Age SAMHSA 2011 GAIN Summary Analytic Data Set (n=29,501)
Homicidal/Suicidal Thoughts by Age SAMHSA 2011 GAIN Summary Analytic Data Set (n=29,469)
Count of Major Clinical Problems at Intake Source: CSAT 2010 AT Summary Analytic Data Set (n=17,978)
Multiple Problems are the Norm Across All age Groups SAMHSA 2011 GAIN Summary Analytic Data Set (n=29,782)
The Elephant in the Room is the Severity of Victimization Source: CSAT 2010 AT Summary Analytic Data Set (n=18,120)
Environmental Strengths Index by Age SAMHSA 2011 GAIN Summary Analytic Data Set (n=27,625)
Unmet Need for Mental Health Treatment by 3 Months Higher for Adolescents and Young Adults Age* * p<.05 SAMHSA 2011 GAIN SA Data Set subset to has 3m Follow up (n=14,358)
Unmet Need for Medical Treatment by 3 Months Significantly higher for Young Adults and Adolescents * p<.05 Age* SAMHSA 2011 GAIN SA Data Set subset to has 3m Follow up (n=8,517)
Relative Percent Change in Abstinence (6 months minus intake/intake) by Age SAMHSA 2011 GAIN SA Data Set subset to 6 Month Follow up (n=20,181)
Change in GPRA Outcomes by Age (Intake to Last Wave*) *Last wave is the last follow-up SAMHSA 2011 GAIN SA Data Set subset to 1+ Follow ups
Change in GPRA Outcomes by Age (Intake to Last Wave*) *Last wave is the last follow-up SAMHSA 2011 GAIN SA Data Set subset to 1+ Follow ups
General Predictors of Bigger Effects • A strong intervention protocol based on prior evidence • Quality assurance to ensure protocol adherence and project implementation • Proactive case supervision of individual • Triage to focus on the highest severity subgroup
Impact of the numbers of these Favorable features on Recidivism in 509 Juvenile Justice Studies in Lipsey Meta Analysis The more features, the lower the recidivism Average Practice Source: Adapted from Lipsey, 1997, 2005
Cognitive Behavioral Therapy (CBT) Interventions that Typically do Better than Usual Practice in Reducing Juvenile Recidivism (29% vs. 40%) • Aggression Replacement Training • Reasoning & Rehabilitation • Moral Reconation Therapy • Thinking for a Change • Interpersonal Social Problem Solving • MET/CBT combinations and Other manualized CBT • Multisystemic Therapy (MST) • Functional Family Therapy (FFT) • Multidimensional Family Therapy (MDFT) • Adolescent Community Reinforcement Approach (ACRA) • Assertive Continuing Care NOTE: There is generally little or no differences in mean effect size between these brand names Source: Adapted from Lipsey et al 2001, Waldron et al, 2001, Dennis et al, 2004
Implementation is Essential (Reduction in Recidivism from .50 Control Group Rate) The best is to have a strong program implemented well The effect of a well implemented weak program is as big as a strong program implemented poorly Thus one should optimally pick the strongest intervention that one can implement well Source: Adapted from Lipsey, 1997, 2005
Change in Abstinence by level of Support: Adolescent Community Reinforcement Approach (A-CRA) Effects associated with Coaching, Certification and Monitoring (OR=7.6) Source: CSAT 2008 SA Dataset subset to 6 Month Follow up (n=1,961) 30
Key Points to Take Away There is a major quality chasm in current practice that are even worse for adolescents and young adults Multiple co-occurring problems are the norm, vary in mix by age and heavily related to victimization and trauma The best predictors of outcome are the use of evidenced based assessment and practice that have worked for others, have strong quality assurance, strong case supervision, and good triage of services to well defined problems.