Download
1 / 54
540 likes | 547 Views
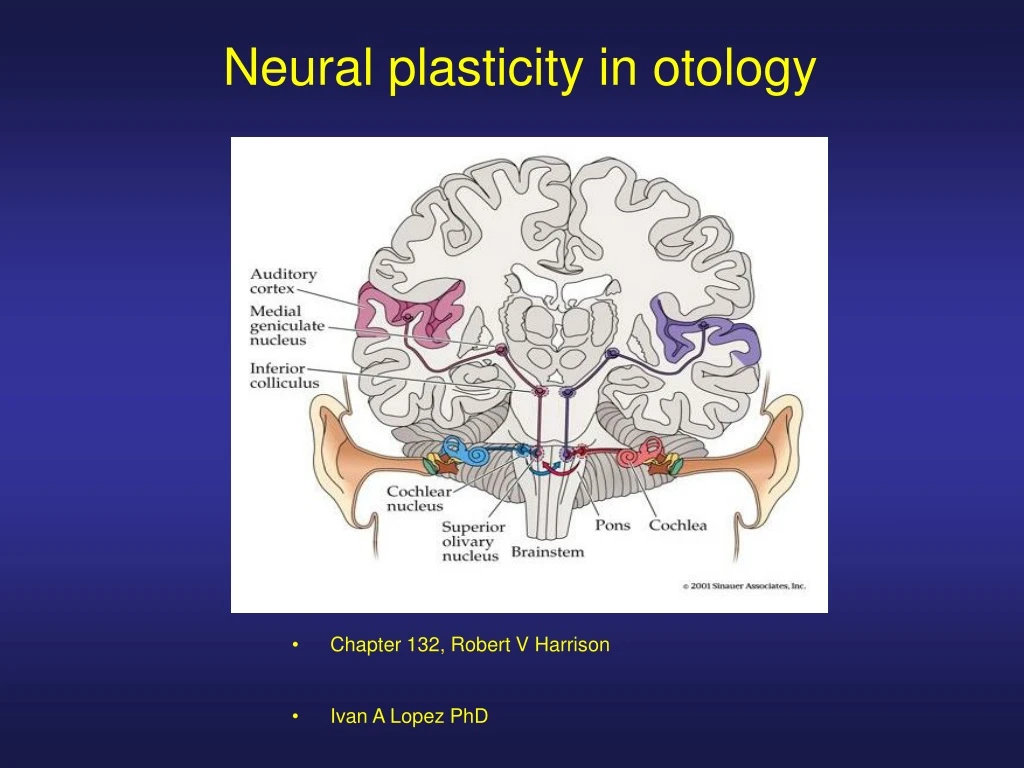
Neural plasticity in otology. Chapter 132, Robert V Harrison Ivan A Lopez PhD. Neural plasticity underlies many clinical events in otology:.

E N D
Neural plasticity in otology Chapter 132, Robert V Harrison Ivan A Lopez PhD
Neural plasticity underlies many clinical events in otology: • a) Adaptation to a vestibular insult, b) rehabilitation after hearing loss, c) auditory learning after a cochlear implant all are mediated by neural rewiring. • Changes in the pattern of peripheral input in the auditory system have effects on central neural organization. After a period of deafness, functional and structural changes occur in the auditory brain. • Neural plasticity is age-related. There is a maximum change in early development. • Early Cochlear implant or hearing aid benefit congenitally deaf child (the earlier the better). • Early detection and diagnosis of hearing cells (neonatal hearing screening).
Definition of Plasticity • Anatomical studies established that plasticity relates to morpho-physiological (cellular and molecular) changes in the brain. • The auditory and vestibular system have the inherent ability to modify or reorganize. • Example Levi-Montalcini experiment (J Comp Neurol 1949, 91;209-242), where anatomical changes of the auditory pathway after experimental lesions to the inner ear were documented. • Cell counts, axonal pathway changes and alteration to neural structure were observed to follow partial or total auditory deafferentation.
Methods to study plastic change • Electrophysiological studies in animal model and humans, functional neuro-imaging studies (PET, functional MRI, magneto-encephalographic studies. • Behavioral studies monitored hearing performance after manipulation of the auditory input. • Observation of improved sensory function over time in patients with hearing or vestibular loss.
Time course of plastic change • Changes to the auditory system occur from minutes, to weeks or months and years. • In acute plasticity auditory neuron receptive fields (excitatory and inhibitory frequency tuning curves) change within 10 minutes after induction of cochlear lesions or partial deafferentation. • Short term plastic changes may occurred but is not clear whether these changes would be consolidated in longer term. • Extensive auditory system reorganization after trauma occur over longer time. • Studies have shown a modification of central tonotopic mapping as a result of cochlear lesion. • The time course of plastic change occurs over many weeks. In some cases extensive reorganization occurred, for example new axonal growth and synaptogenesis have occurred.
Age related plasticity • Reorganization of tonotopic maps after cochlear lesions is significantly different when experimental manipulation is done in the neonate compared with the adult animal. • Example: performance of a congenitally deaf child provided with a cochlear implant at an early age compared with a deaf child implanted a much later age.
Reorganization of central tonotopic maps after cochlear lesions • Tonotopic maps can be considered the mainline organizational feature of the auditory system. • These projections are called cochleo-topic (or tonotopic), given the place coding of sound frequency along the cochlear length.
Tonotopic map in normal cat auditory cortex as determined by microelectrode recordings 3 neurons Isofrequency contours are imaginary planes that connect the positions of all the cells having similar frequencies Aef: anterior ectosylvian fissure; pef, posterior ectosylvian fissure; sf: sylvian fissure
What are the plastic changes in the tonotopic map after ototoxic treatment? • There is a reorganization of the tonotopic map. • Age, time and dose dependent, degree of cochlear damage.
Tonotopic map reorganization in a developmental model after ototoxic treatment (cat) • Amikacin was given systemically, cochlear lesions were bilaterally symmetric • ABR shows hat the basal region of the cochlea was damaged, but apical areas (6-8kHz region) were preserved. • The cortical tonotopic map is characterized by a normal representation of low frequencies, but the cortical region deprived of normal input now contains neurons tuned to 6-8 kHz
Cortical tonotopic maps in a cat with neonatal basal cochlear lesion The cochlear lesion was more extensive With a severe basal region and hair cell loss at the apical region The ABR slopes down across al frequencies This animal developed a cortical frequency map in which all neurons have a common 6.6 kHz frequency tuning The low frequency region is severely distorted
Cortical frequency map reorganization in adult chinchilla after ototoxic treatment • Normal tonotopic map • Cochlear lesion. A typical finding overrepresentation of neurons with • frequency 2.5-3.5kHz
Conclusions • Modification to cortical frequency maps are the result of neural rewiring. • The excitatory receptive fields of neurons tuned to the common frequency are similar in shape. • They have similar minimum thresholds and bandwidths
Adult versus developmental plasticity of sensory systems • At the auditory cortex there seems to be a pattern of reorganization of tonotopic maps after cochlear lesions in the developing neonate similar to that of adult animal. • Tonotopic maps in sub-cortical auditory nuclei show significant differences in map reorganization after lesion in a developmental model compared with mature subjects. • At sub-cortical levels there is evidence of age-related plasticity.
Tonotopic map reorganization at subcortical levels (IC) • What are the changes in the subcortical levels (inferior colliculus). • In normal conditions the tonotopic maps shows an orderly progression of the neuron characteristics frequency . • After cochlear lesion in the neonate there is normal octave-spaced frequency up to 10 kHz, at more ventral areas there is large region containing identically tuned neurons.
Tonotopic map reorganization at subcortical levels (IC) • Normal tonotopic map of the chinchilla inferior colliculus.
Tonotopic maps of the chinchilla inferior colliculus after ototoxic treatment There is a normal octave-spaced frequency contours within the IC up to 10 KHz. There is a large region containing identically tuned neurons Amikacin 3 days Maps derived from single neuron recordings in electrode tracks along the dorso-ventral axis of the IC
Conclusions • These studies establish that tonotopic map reorganization occurs at low levels in the auditory pathway after basal cochlear lesions induced in early postnatal period. • In adults partial cochlear deaferentation produces no reorganization at the level of the cochlear nucleus.
Salient aspects of developmental and adult plasticity experiments
Early development Neural projections between levels have considerable divergence throughout the system Dynamic cellular and molecular changes occur at this stage
Adult Normally developed projection system Normal point to point cochleotopic projection System from the cochlea to the auditory cortex
Developmental plasticity after lesion Cochlear lesion induced Neonatally At the level of the auditory cortex and at the midbrain, deaferented areas contain neurons that seem to be connected to common points along the cochlea
Adult plasticity Cochlear lesions induced in an adult Very little evidence of frequency maps reorganization have been seen. Rewiring to produce overrepresentation is confined to the cortex
Tonotopic maps after long-term local excitation of the cochlea • What happen when there is augmented cochlear afferent activity?
Experiment • Cats were reared in an environment where an 8-kHz acoustic signal was constantly present (55 to 60db). The 8kHZ tone was frequency modulated to avoid adaptative effects and hair cell damage. • Six months after tonotopic maps were created.
Tonotopic maps in the auditory cortex of a cat Frequency map from normal control The 8 to 16 kHz octave interval is shaded to Emphasize the main difference between subjects Cat that spent 1 month post-natally in an acoustic environment with a constant 8-KHz signal. Bottom (A) normal point to point normal organization (B) Increase firing rate of a group of midcochlear neurons
Conditions for plasticity in the adult cortex • Plasticity of sensory cortex occurs after repeated chronic exposure to well specified stimuli. • Plastic changes are evident only if the sensory stimulus as behavioral significance to the animal. • Long term changes in the auditory neuron receptive field are induced in tonal stimulation associated to various behavioral conditioning tasks. • A model was proposed that the nucleus basalis the source of cholinergic projections to the sensory cortex has important role in plastic modifications to cortical networks. • The developing system maybe significant different. • Passive overstimulation can result in the development of a modified map.
Animal models of deafness and effects of cochlear implant electrical stimulation • A wide range of structural and functional changes have been observed in the auditory system in association with experimental and naturally occurring deafness. • Important question relates whether stimulation with a cochlear implant can serve to restore critical features of auditory function such as synaptic integrity.
Studies of cochlear electrical stimulation in animal models of deafness • Auditory terminal endings in deaf cats exhibit morphological abnormalities that are partially reversible with restored activity with cochlear implantation. • There are positive effects of electrical stimulation on auditory brain stem nuclei, midbrain and auditory cortex. • Results suggest that there is a critical period or at least age-related plasticity for the developing auditory cortex
Basic mechanism of plastic change • Neural reorganization is the result of several mechanism. • The behavior of underused neurons depends on the establishment of synaptic connections, the pruning of underused synapses, and the strength of individual connections. • External neural and hormonal factors can facilitate plastic change.
Some mechanisms present during development may not play important role in the mature brain. • Initial connections involved chemotropic guidance and myelination processes, are not present in the mature brain. • Drastic pruning of interneuronal connections do not occur in the adult. • Thus the mechanism of plasticity are different during development and the adult brain.
As seen before during neonatal period the divergent innervation pattern develops into the normal point to point projection systems. • Many mechanism are likely involved in this process. • Growing neurons are making connections with target cells and there is a physical space competition such that neurons that are most proximal win out. • Synaptic strengthening through long-term potentiation strength the most directed connections and promote their survival. • Sound-driven neural activity likely is more influential in the formation of the adult connectivity. • This is the case if synaptic strength follow Hebbian rules,
Robust strengthening of connections between neurons is achieved under conditions where patterns of pre-synaptic and postsynaptic activity are highly correlated. • This is the case for an acoustic stimuli that drives identical patterns in neighboring cell groups.
Tonotopic map reorganization in the developing subject Auditory projection resulting from basal cochlea lesion during early developmental period, At the AC and MB deaferented areas contain neurons connected to a common point along the cochlea. A mechanism to explain this is that divergent neural projections are not eliminated because in the adjacent deafferented region there are not neurons competing for target cells There is always a small degree of divergence associated with tonotopic projections
Cortical map plasticity in adult subjects This map represent changes after cochlear lesion in a mature animal Little evidence of frequency map reorganization is found at the subcortical levels Rewiring to produce overrepresentation is confined to the thalamocortex, Two mechanisms 1) Alteration of preexisting neural connections 2) Nerve growth processes such as neurogenesis, axon sprouting and synaptogenesis.
Conclusion • In the auditory cortex and thalamus there is some degree of divergent input. There are laterally connecting local interneurons and there are larger interneuronal connections • They are normally inhibited. • Local deaferentation release that inhibition unmasking of existing lateral connections
Cellular level mechanism of plasticity Post-tetanic potentiation: A presynaptic neuron excites a second neuron, repeated presynaptic modulation result in an increased effectiveness of the synapse that is maintained for some time. The theory behind short –term plasticity is that it is caused by presynaptic Ca2+ accumulation that enhances neurotransmitter release
Long term potentiation • Long term modifications of synapses could be experimentally induced. • LTP can result from a repeated activation f the synapse. • LTP exist ubiquitously in the brain. • NMDA receptor is involved in LTP. • NMDA receptor is a fast ionotropic ion channel activated by glutamate. • Synapses with NMDA receptor can develop LTP but not when the receptor is blocked.
The key aspect of the NMDA receptor is that its ion channel has a voltage –dependent Mg2+ block that can alter the cell excitability, by controlling Ca2+ permeability . • The metabotopic glutamate receptor can also be involved in LTP.
Hebb’s Postulate • Synaptic systems involving NMDA receptor frequently follow hebbian rules. • In 1949 Hebbs postulate that when an axon of cell A is near to excite cell B and repeatedly or persistently takes part in firing it, some growth process or metabolic change takes place in one or both cells such that A efficiency as one of the cells firing B is increased. • “Cells that fire together, wire together” Acoustic stimulation results in groups of neurons in ascending arrays with highly correlated activity. Important condition for establishing and maintaining tonotopicity
When Neuron A talks to Neuron B, glutamate binds to the NMDA channel and opens it. No LTP occurs because the magnesium ion blocks the channel! If Neuron B is activated, magnesium unblocks the channel but since Neuron A is not active, no glutamate is bound and the channel does not open. Only when both Neuron A and Neuron B are activated does the NMDA receptor become activated: magnesium unblocks the channel and glutamate opens the channel. In this way, the NMDA receptor acts as a “coincidence detector” that detects the simultaneous activation of both Neuron A and Neuron B. As Donald Hebb hypothesized, when both neurons are activated at the same time, their connections are strengthened
Pre and postsynaptic mechanism for enhancing synaptic efficacy 1 More synaptic vesicles 2 Increase in the number of release sites 3 Potentiation of a release by increase vesicle available for release 4 Increase in the sensitivity of existing postsynaptic receptors 5 Increase number of receptors 6 Synaptogenesis
Practical Issues relating to neural plasticity in otology • Hearing loss in infants: hearing loss during early development may negatively affect central development. • There is a critical period during which cochlear function needs to be particularly intact. • Mild hearing loss, chronic conductive hearing loss, and bilaterally asymmetric hearing loss may alter normal central pathway development.
Neonatal hearing disorders that might lead to problems in language development become evident 4 or 5 years later when such development can be assessed. • The best practical strategy is to have early detection of hearing problems through neonatal or infant hearing screening programs and subsequent early intervention with hearing aids, cochlea implants and auditory habilitation training.
Experiments in deaf children with cochlear implants • Average post-implantation performance on standard speech understanding test. • All children were prelingually (congenitally) deaf, the population was homogeneous in terms of degree of residual hearing , school settings and access to rehabilitation therapy.
The data set has been divided into children implanted at an early age compared with children impaired later. • On average children implanted at a young age eventually outperform others. • Similar conclusions are reached in other interventions outcome studies in vision, sensory motor training and education
The influence of age at implantation on speech hearing tests in congenitally or prelingually deaf children Test of auditory comprehension Word intelligibility by picture identification (WIPI) Glendonal auditory screening procedure (GASP)
Conclusions • Compensation for any neural deficit is best achieved by early intervention. • Central auditory system development is guided by cochlear activity patterns. • A cochlear implant provided to a young infant would aid hearing but also the augmented stimulation of the system would have an influence on central development.